

Prostaglandin D₂: a dominant mediator of aspirin-exacerbated respiratory disease
- PMID: 25218285
- PMCID: PMC4289104
- DOI: 10.1016/j.jaci.2014.07.031
Prostaglandin D₂: a dominant mediator of aspirin-exacerbated respiratory disease
Abstract
Background: Aspirin desensitization followed by high-dose aspirin therapy is routinely performed for patients with aspirin-exacerbated respiratory disease (AERD). Little is known about the contributions of mediators other than cysteinyl leukotrienes to aspirin reactions and to the therapeutic benefit of high-dose aspirin therapy.
Objective: We investigated differences in urinary eicosanoid metabolite levels and blood eosinophil counts in patients with AERD who tolerate and those who fail aspirin desensitization and also in patients with AERD who were successfully treated with high-dose aspirin therapy.
Methods: Twenty-nine patients with AERD were stratified into those who tolerated aspirin desensitization (group I) and those who did not (group II). Urine was analyzed for eicosanoid metabolites at baseline, during aspirin reactions, and during high-dose aspirin therapy. Blood was analyzed for cell differentials at baseline and during aspirin therapy.
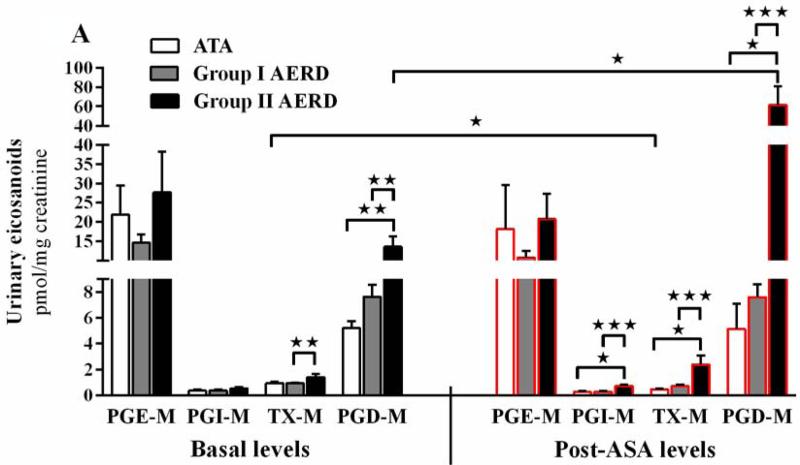
Results: Basal prostaglandin D2 metabolite (PGD-M; 13.6 ± 2.7 vs 7.0 ± 0.8 pmol/mg creatinine [Cr], P < .05) and thromboxane metabolite (TX-M; 1.4 ± 0.3 vs 0.9 ± 0.1 pmol/mg Cr, P < .01) levels were higher in group II than in group I. During aspirin reactions, PGD-M levels remained unchanged, whereas TX-M levels (0.7 ± 0.1 pmol/mg Cr, P = .07) tended to decrease in group I. In contrast, PGD-M levels increased dramatically in group II (61.3 ± 19.9 pmol/mg Cr, P < .05), whereas TX-M levels did not change. The decrease in FEV1 inversely correlated with basal urinary levels of both leukotriene E4 and PGD-M. Blood eosinophil and basophil levels increased and urinary PGD-M levels (2.2 ± 0.8 pmol/mg Cr, P < .001) decreased on 2 months of high-dose aspirin therapy in group I.
Conclusion: Failure to tolerate aspirin desensitization in a subset of patients with AERD is associated with prostaglandin D2 overproduction. The increase in blood eosinophil and basophil counts during high-dose aspirin therapy might reflect the functional consequences of decreased prostaglandin D2 release and the therapeutic benefit of aspirin.
Keywords: Aspirin-exacerbated respiratory disease; Samter triad; aspirin desensitization; asthma; cysteinyl leukotrienes; eosinophils; nasal polyps; prostaglandin D(2); thromboxane; urinary eicosanoids.
Copyright © 2014 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures







References
-
- Kupczyk M, Kurmanowska Z, Kuprys-Lipinska I, Bochenska-Marciniak M, Kuna P. Mediators of inflammation in nasal lavage from aspirin intolerant patients after aspirin challenge. Respiratory Medicine. 2010;104:1404–09. - PubMed
-
- Sladek K, Szczeklik A. Cysteinyl leukotrienes overproduction and mast cell activation in aspirin-provoked bronchospasm in asthma. Eur Respir J. 1993;6:391–99. - PubMed
-
- Stevenson DD, Simon RA, Mathison DA. Aspirin-sensitive asthma: tolerance to aspirin after positive oral aspirin challenges. J Allergy Clin Immunol. 1980;66(1):82–8. - PubMed
-
- Swierczynska-Krepa M, Sanak M, Bochenek Grazyna, Strek P, Cmiel A, Gielicz A, Plutecka H, Szczeklik, Nizankowska-Mogilnicka E. Aspirin desensitization in patients with aspirin-induced and aspirin-tolerant asthma: A double-blind study. J Allergy Clin Immunol. 2014 epub April 25, 2014. - PubMed
-
- Nicholson DW, Ali A, Vaillancourt JP, Calaycay JR, Mumford RA, Zamboni RJ, Ford-Hutchinson AW. Purification to homogeneity and the N-terminal sequence of human leukotriene C4 synthase: a homodimeric glutathione S-transferase composed of 18-kDa subunits. Proc Natl Acad Sci U S A. 1993;90:2015–9. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
