

Systemic safety of bevacizumab versus ranibizumab for neovascular age-related macular degeneration
- PMID: 25220133
- PMCID: PMC4262120
- DOI: 10.1002/14651858.CD011230.pub2
Systemic safety of bevacizumab versus ranibizumab for neovascular age-related macular degeneration
Abstract
Background: Neovascular age-related macular degeneration (AMD) is the leading cause of legal blindness in elderly populations of industrialised countries. Bevacizumab (Avastin®) and ranibizumab (Lucentis®) are targeted biological drugs (a monoclonal antibody) that inhibit vascular endothelial growth factor, an angiogenic cytokine that promotes vascular leakage and growth, thereby preventing its pathological angiogenesis. Ranibizumab is approved for intravitreal use to treat neovascular AMD, while bevacizumab is approved for intravenous use as a cancer therapy. However, due to the biological similarity of the two drugs, bevacizumab is widely used off-label to treat neovascular AMD.
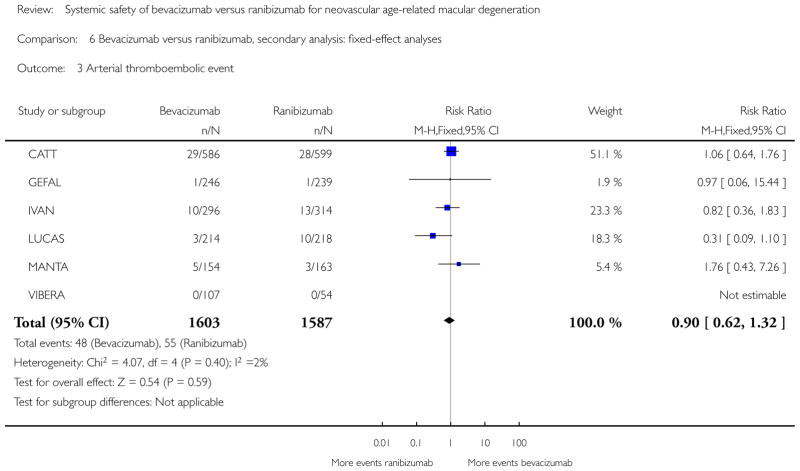
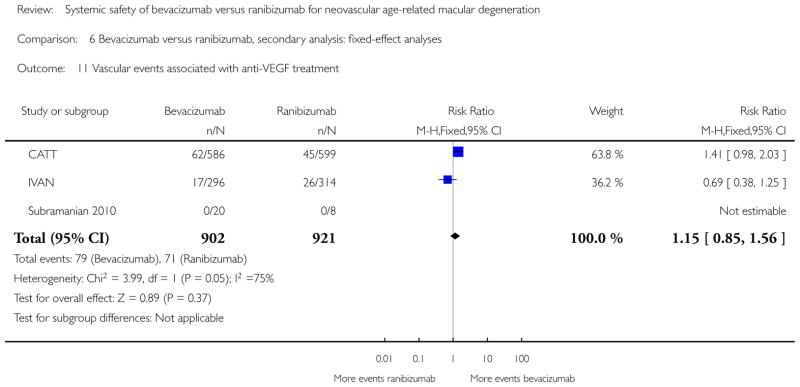
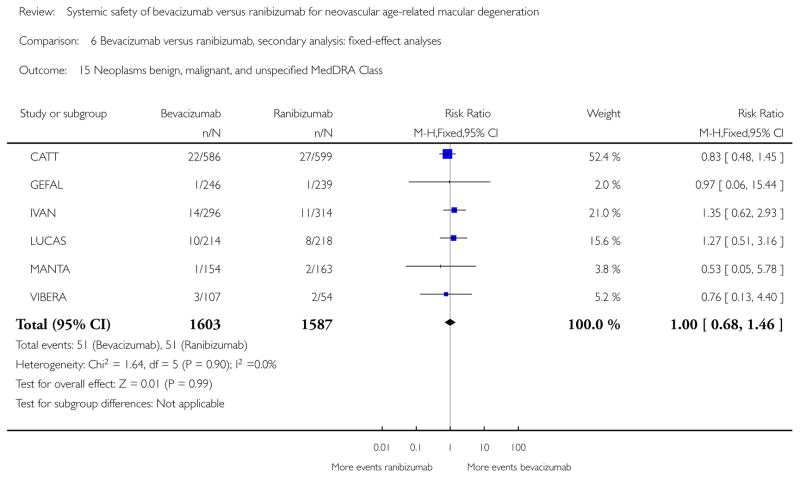
Objectives: To assess the systemic safety of intravitreal bevacizumab (brand name Avastin®; Genentech/Roche) compared with intravitreal ranibizumab (brand name Lucentis®; Novartis/Genentech) in people with neovascular AMD. Primary outcomes were death and All serious systemic adverse events (All SSAEs), the latter as a composite outcome in accordance with the International Conference on Harmonisation Good Clinical Practice. Secondary outcomes examined specific SSAEs: fatal and non-fatal myocardial infarctions, strokes, arteriothrombotic events, serious infections, and events grouped in some Medical Dictionary for Regulatory Activities System Organ Classes (MedDRA SOC). We assessed the safety at the longest available follow-up to a maximum of two years.
Search methods: We searched CENTRAL, MEDLINE, EMBASE and other online databases up to 27 March 2014. We also searched abstracts and clinical study presentations at meetings, trial registries, and contacted authors of included studies when we had questions.
Selection criteria: Randomised controlled trials (RCTs) directly comparing intravitreal bevacizumab (1.25 mg) and ranibizumab (0.5 mg) in people with neovascular AMD, regardless of publication status, drug dose, treatment regimen, or follow-up length, and whether the SSAEs of interest were reported in the trial report.
Data collection and analysis: Two authors independently selected studies and assessed the risk of bias for each study. Three authors independently extracted data.We conducted random-effects meta-analyses for the primary and secondary outcomes. We planned a pre-specified analysis to explore deaths and All SSAEs at the one-year follow-up.
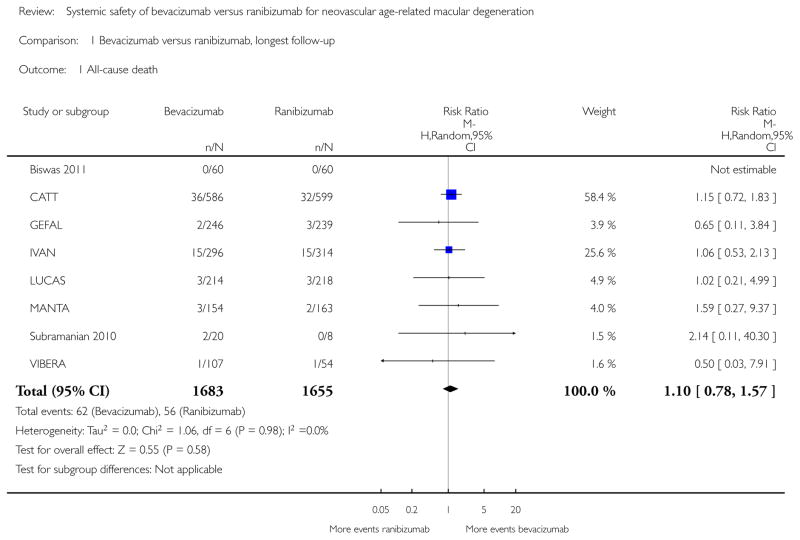
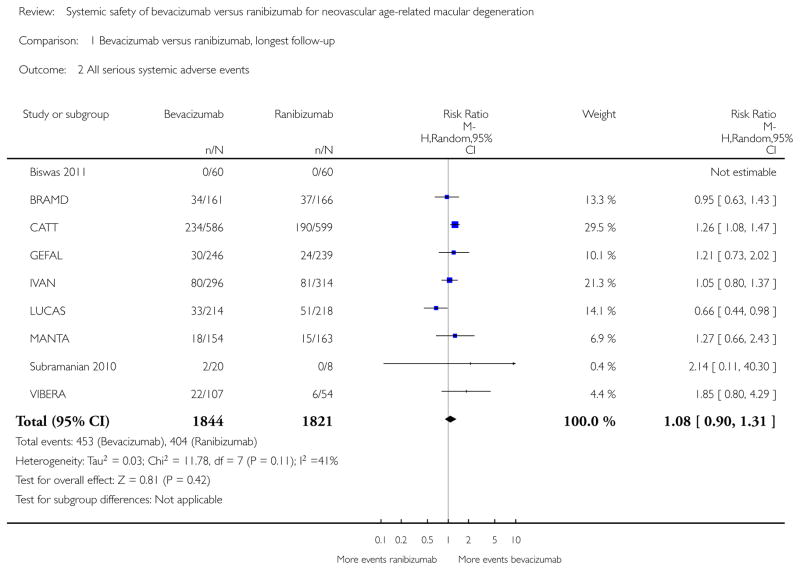
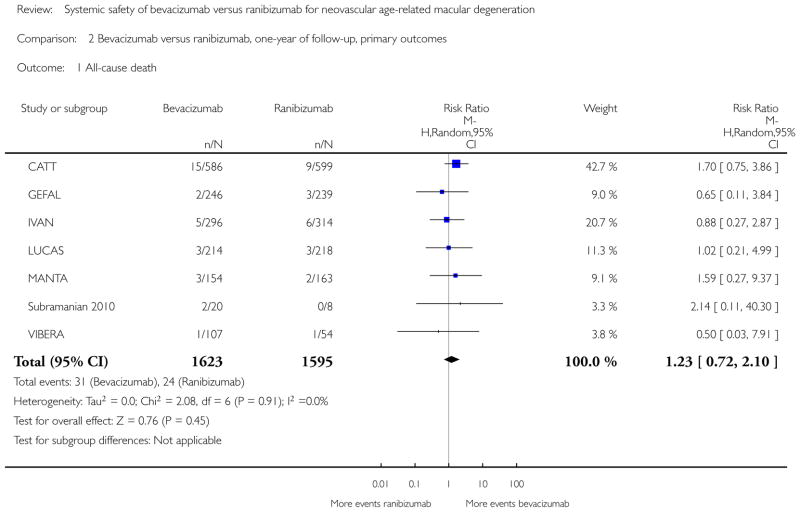
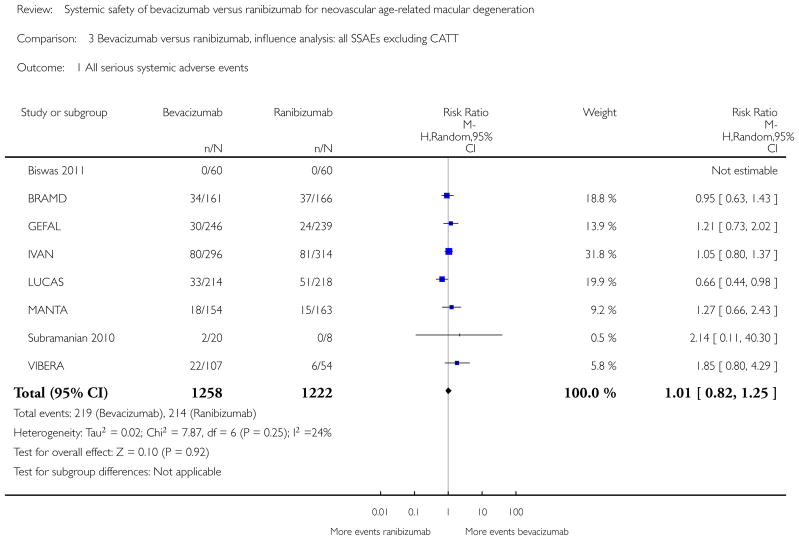
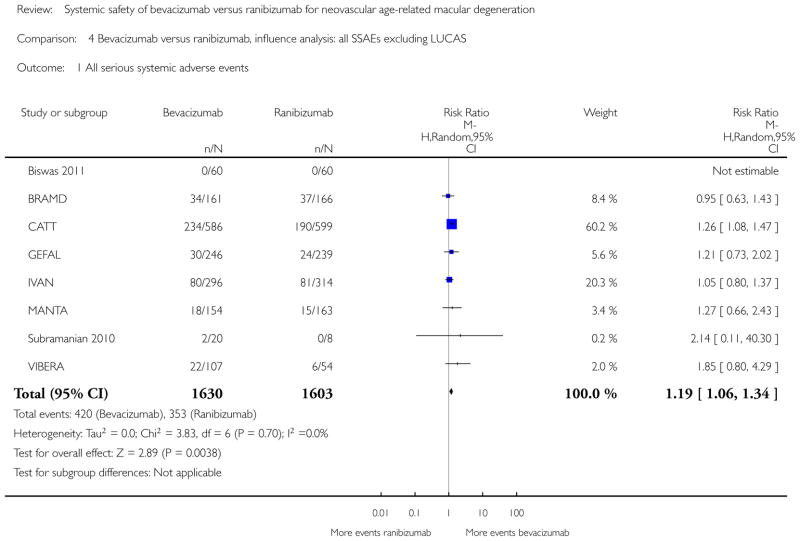
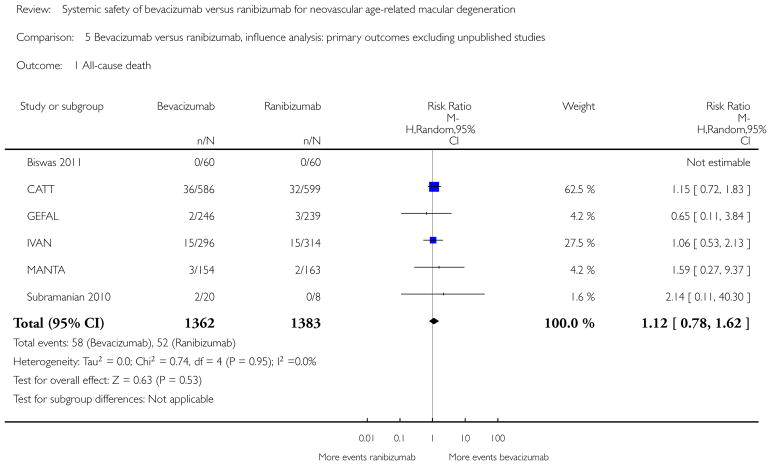
Main results: We included data from nine studies (3665 participants), including six published (2745 participants) and three unpublished (920 participants) RCTs, none supported by industry. Three studies excluded participants at high cardiovascular risk, increasing clinical heterogeneity among studies. The studies were well designed, and we did not downgrade the quality of the evidence for any of the outcomes due to risk of bias. Although the estimated effects of bevacizumab and ranibizumab on our outcomes were similar, we downgraded the quality of the evidence due to imprecision.At the maximum follow-up (one or two years), the estimated risk ratio (RR) of death with bevacizumab compared with ranibizumab was 1.10 (95% confidence interval (CI) 0.78 to 1.57, P value = 0.59; eight studies, 3338 participants; moderate quality evidence). Based on the event rates in the studies, this gives a risk of death with ranibizumab of 3.4% and with bevacizumab of 3.7% (95% CI 2.7% to 5.3%).For All SSAEs, the estimated RR was 1.08 (95% CI 0.90 to 1.31, P value = 0.41; nine studies, 3665 participants; low quality evidence). Based on the event rates in the studies, this gives a risk of SSAEs of 22.2% with ranibizumab and with bevacizumab of 24% (95% CI 20% to 29.1%).For the secondary outcomes, we could not detect any difference between bevacizumab and ranibizumab, with the exception of gastrointestinal disorders MedDRA SOC where there was a higher risk with bevacizumab (RR 1.82; 95% CI 1.04 to 3.19, P value = 0.04; six studies, 3190 participants).Pre-specified analyses of deaths and All SSAEs at one-year follow-up did not substantially alter the findings of our review.Fixed-effect analysis for deaths did not substantially alter the findings of our review, but fixed-effect analysis of All SSAEs showed an increased risk for bevacizumab (RR 1.12; 95% CI 1.00 to 1.26, P value = 0.04; nine studies, 3665 participants): the meta-analysis was dominated by a single study (weight = 46.9%).The available evidence was sensitive to the exclusion of CATT or unpublished results. For All SSAEs, the exclusion of CATT moved the overall estimate towards no difference (RR 1.01; 95% CI 0.82 to 1.25, P value = 0.92), while the exclusion of LUCAS yielded a larger RR, with more SSAEs in the bevacizumab group, largely driven by CATT (RR 1.19; 95% CI 1.06 to 1.34, P value = 0.004). The exclusion of all unpublished studies produced a RR of 1.12 for death (95% CI 0.78 to 1.62, P value = 0.53) and a RR of 1.21 for SSAEs (95% CI 1.06 to 1.37, P value = 0.004), indicating a higher risk of SSAEs in those assigned to bevacizumab than ranibizumab.
Authors' conclusions: This systematic review of non-industry sponsored RCTs could not determine a difference between intravitreal bevacizumab and ranibizumab for deaths, All SSAEs, or specific subsets of SSAEs in the first two years of treatment, with the exception of gastrointestinal disorders. The current evidence is imprecise and might vary across levels of patient risks, but overall suggests that if a difference exists, it is likely to be small. Health policies for the utilisation of ranibizumab instead of bevacizumab as a routine intervention for neovascular AMD for reasons of systemic safety are not sustained by evidence. The main results and quality of evidence should be verified once all trials are fully published.
Conflict of interest statement
Some of the review authors are trial investigators on the studies included in this review.
Figures































References
References to studies included in this review
-
- Schauwvlieghe A-SM, Dijkman G, Hooymans JM, Verbraak FD, Dijkgraaf MG, Peto T, et al. Comparing the effectiveness of bevacizumab to ranibizumab in patients with exudative age-related macular degeneration. BRAMD. Investigative Ophthalmology and Visual Science. 2014;55 ARVO E-Abstract 870. - PMC - PubMed
-
- Martin DF, Maguire MG, Fine SL, Ying GS, Jaffe GJ, Grunwald JE, et al. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two-year results. Ophthalmology. 2012;119(7):1388–98. - PMC - PubMed
- Martin DF, Maguire MG, Ying GS, Grunwald JE, Fine SL, Jaffe GJ. Ranibizumab and bevacizumab for neovascular age-related macular degeneration. New England Journal of Medicine. 2011;364(20):1897–908. - PMC - PubMed
-
- Kodjikian L, Souied EH, Mimoun G, Mauget-Faysse M, Behar-Cohen F, Decullier E, et al. Ranibizumab versus bevacizumab for neovascular age-related macular degeneration: results from the GEFAL noninferiority randomized trial. Ophthalmology. 2013;120(11):2300–9. - PubMed
-
- Chakravarthy U, Harding SP, Rogers CA, Downes SM, Lotery AJ, Culliford LA, et al. Alternative treatments to inhibit VEGF in age-related choroidal neovascularisation: 2-year findings of the IVAN randomised controlled trial. Lancet. 2013;382(9900):1258–67. - PubMed
- Chakravarthy U, Harding SP, Rogers CA, Downes SM, Lotery AJ, Wordsworth S, et al. Ranibizumab versus bevacizumab to treat neovascular age-related macular degeneration: one-year findings from the IVAN randomized trial. Ophthalmology. 2012;119(7):1399–411. - PubMed
Additional references
-
- Bassler D, Montori VM, Briel M, Glasziou P, Walter SD, Ramsay T, et al. Reflections on meta-analyses involving trials stopped early for benefit: is there a problem and if so, what is it? Statistical Methods in Medical Research. 2013;22(2):159–68. - PubMed
References to other published versions of this review
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical