

Dietary sodium restriction: a neglected therapeutic opportunity in chronic kidney disease
- PMID: 25222815
- PMCID: PMC4189688
- DOI: 10.1097/MNH.0000000000000073
Dietary sodium restriction: a neglected therapeutic opportunity in chronic kidney disease
Abstract
Purpose of review: Restriction of dietary sodium is recommended at a population level as well as for groups at high cardiovascular risk, and chronic kidney disease (CKD). This review addresses recent evidence for the protective effect of dietary sodium restriction in CKD patients specifically.
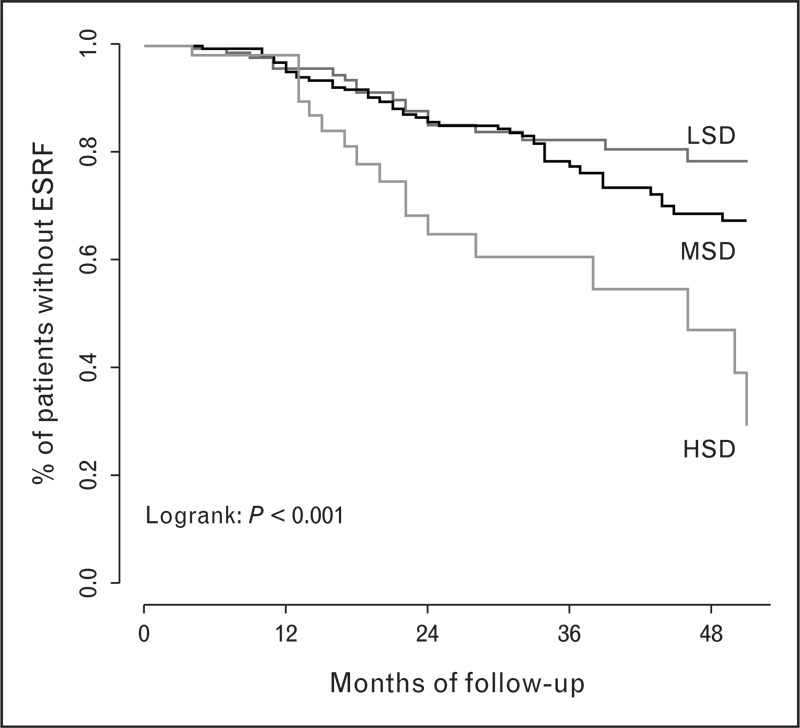
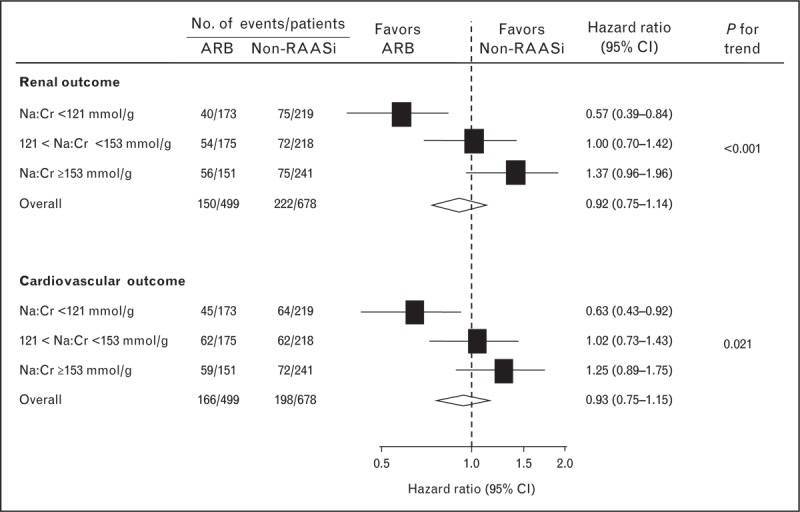
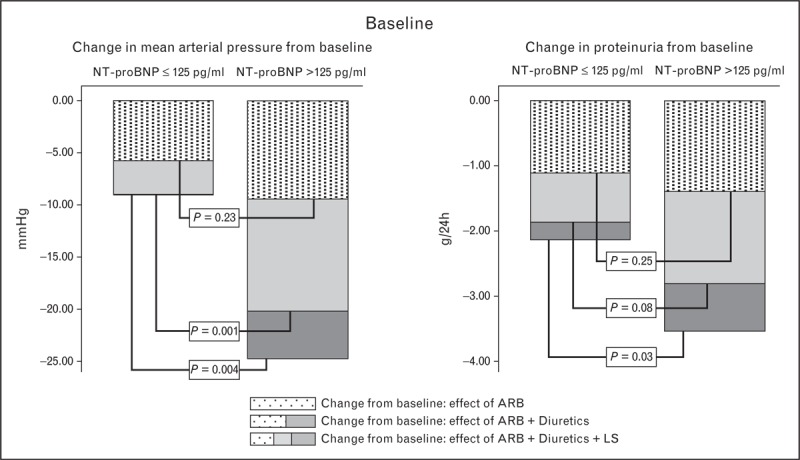
Recent findings: Sodium intake in CKD populations is generally high, and often above population average. Recent data demonstrated that moderately lower sodium intake in CKD patients is associated with substantially better long-term outcome of renin-angiotensin-aldosterone system (RAAS)-blockade, in diabetic and nondiabetic CKD, related to better effects of RAAS-blockade on proteinuria, independent of blood pressure. This is in line with better short-term efficacy of RAAS-blockade during moderate sodium restriction in diabetic and nondiabetic CKD. This effect of sodium restriction is likely mediated by its effects on volume status. Sustainable sodium restriction can be achieved by approaches on the basis of behavioral sciences.
Summary: Moderate restriction of dietary sodium can substantially improve the protective effects of RAAS-blockade in CKD, by specific renal effects apparent from proteinuria reduction. The latter precludes straightforward extrapolation of data from nonrenal populations to CKD. Concerns regarding the adverse effects of a very low sodium intake should not distract from the protective effects of moderate sodium restriction. Prospective studies should assess the efficacy and sustainability of different strategies to target high sodium intake in CKD, along with measures at population level.
Video abstract: http://links.lww.com/CONH/A14.
Figures


References
-
- Beaglehole R, Bonita R, Horton R, et al. Priority actions for the noncommunicable disease crisis. Lancet 2011; 377:1438–1447 - PubMed
-
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int 2013; 3:1–150 - PubMed
-
- Lambers Heerspink HJ, Holtkamp FA, Parving HH, et al. Moderation of dietary sodium potentiates the renal and cardiovascular protective effects of angiotensin receptor blockers. Kidney Int 2012; 82:330–337 - PubMed
-
- Kwakernaak AJ, Krikken JA, Binnenmars SH, et al. Effects of sodium restriction and hydrochlorothiazide on RAAS blockade efficacy in diabetic nephropathy: a randomised clinical trial. Lancet Diabetes Endocrinol 2014; 2:385–395 - PubMed
-
First intervention trial showing the effects of sodium restriction, diuretic, and their combination in patients with diabetes and nephropathy on RAAS-blockade. Moderate dietary sodium restriction considerably increased the efficacy of RAAS-blockade. This article also reports on sodium excretion in the unselected recruitment population, showing that sodium intake in this outpatient population of patients with diabetes and nephropathy was considerably above the population average in The Netherlands.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
