

Retrocrural space involvement on computed tomography as a predictor of mortality and disease severity in acute pancreatitis
- PMID: 25222846
- PMCID: PMC4164622
- DOI: 10.1371/journal.pone.0107378
Retrocrural space involvement on computed tomography as a predictor of mortality and disease severity in acute pancreatitis
Abstract
Background: Because computed tomography (CT) has advantages for visualizing the manifestation of necrosis and local complications, a series of scoring systems based on CT manifestations have been developed for assessing the clinical outcomes of acute pancreatitis (AP), including the CT severity index (CTSI), modified CTSI, etc. Despite the internationally accepted CTSI having been successfully used to predict the overall mortality and disease severity of AP, recent literature has revealed the limitations of the CTSI. Using the Delphi method, we establish a new scoring system based on retrocrural space involvement (RCSI), and compared its effectiveness at evaluating the mortality and severity of AP with that of the CTSI.
Methods: We reviewed CT images of 257 patients with AP taken within 3-5 days of admission in 2012. The RCSI scoring system, which includes assessment of infectious conditions involving the retrocrural space and the adjacent pleural cavity, was established using the Delphi method. Two radiologists independently assessed the RCSI and CTSI scores. The predictive points of the RCSI and CTSI scoring systems in evaluating the mortality and severity of AP were estimated using receiver operating characteristic (ROC) curves.
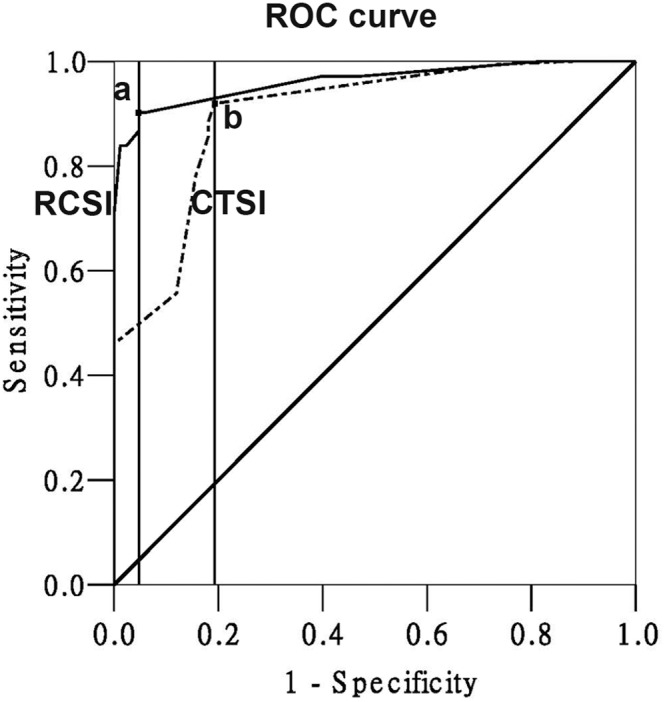
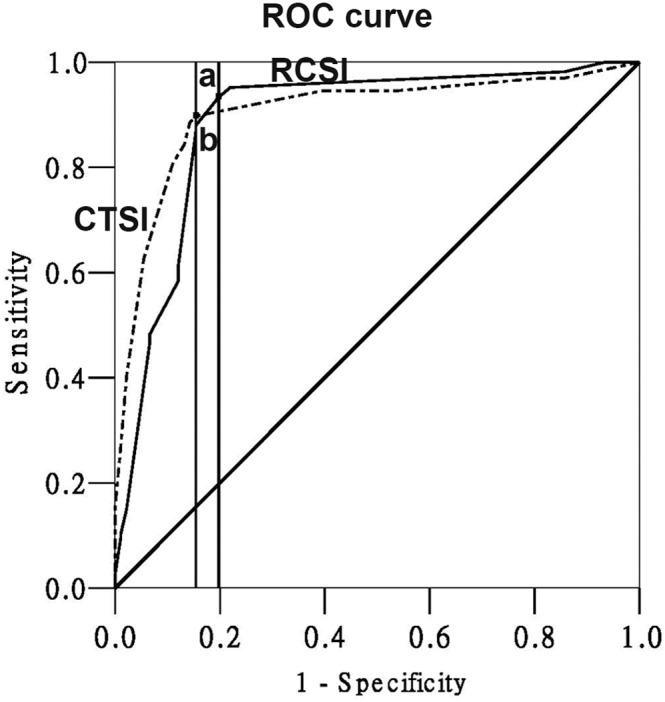
Principal findings: The RCSI score can accurately predict the mortality and disease severity. The area under the ROC curve for the RCSI versus CTSI score was 0.962±0.011 versus 0.900±0.021 for predicting the mortality, and 0.888±0.025 versus 0.904±0.020 for predicting the severity of AP. Applying ROC analysis to our data showed that a RCSI score of 4 was the best cutoff value, above which mortality could be identified.
Conclusion: The Delphi method was innovatively adopted to establish a scoring system to predict the clinical outcome of AP. The RCSI scoring system can predict the mortality of AP better than the CTSI system, and the severity of AP equally as well.
Conflict of interest statement
Figures
References
-
- Balthazar EJ (2002) Complications of acute pancreatitis: clinical and CT evaluation. Radiol Clin North Am 40: 1211–1227. - PubMed
-
- Lenhart DK, Balthazar EJ (2008) MDCT of acute mild (nonnecrotizing) pancreatitis: abdominal complications and fate of fluid collections. American Journal of Roentgenology 190: 643–649. - PubMed
-
- Balthazar EJ, Freeny PC, vanSonnenberg E (1994) Imaging and intervention in acute pancreatitis. Radiology 193: 297–306. - PubMed
-
- Mortele KJ, Wiesner W, Intriere L, Shankar S, Zou KH, et al. (2004) A modified CT severity index for evaluating acute pancreatitis: improved correlation with patient outcome. AJR Am J Roentgenol 183: 1261–1265. - PubMed
-
- De Waele JJ, Delrue L, Hoste EA, De Vos M, Duyck P, et al. (2007) Extrapancreatic inflammation on abdominal computed tomography as an early predictor of disease severity in acute pancreatitis: evaluation of a new scoring system. Pancreas 34: 185–190. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
