

Rehabilitation nutrition for sarcopenia with disability: a combination of both rehabilitation and nutrition care management
- PMID: 25223471
- PMCID: PMC4248414
- DOI: 10.1007/s13539-014-0162-x
Rehabilitation nutrition for sarcopenia with disability: a combination of both rehabilitation and nutrition care management
Abstract
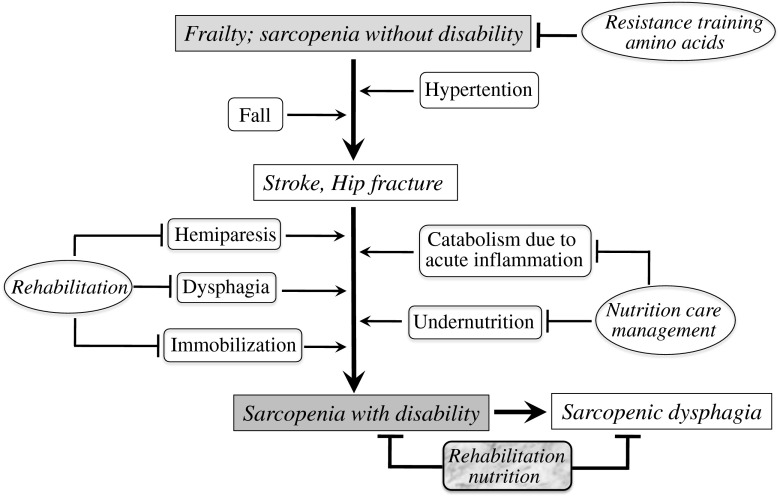
Malnutrition and sarcopenia often occur in rehabilitation settings. The prevalence of malnutrition and sarcopenia in older patients undergoing rehabilitation is 49-67 % and 40-46.5 %, respectively. Malnutrition and sarcopenia are associated with poorer rehabilitation outcome and physical function. Therefore, a combination of both rehabilitation and nutrition care management may improve outcome in disabled elderly with malnutrition and sarcopenia. The concept of rehabilitation nutrition as a combination of both rehabilitation and nutrition care management and the International Classification of Functioning, Disability and Health guidelines are used to evaluate nutrition status and to maximize functionality in the elderly and other people with disability. Assessment of the multifactorial causes of primary and secondary sarcopenia is important because rehabilitation nutrition for sarcopenia differs depending on its etiology. Treatment of age-related sarcopenia should include resistance training and dietary supplements of amino acids. Therapy for activity-related sarcopenia includes reduced bed rest time and early mobilization and physical activity. Treatment for disease-related sarcopenia requires therapies for advanced organ failure, inflammatory disease, malignancy, or endocrine disease, while therapy for nutrition-related sarcopenia involves appropriate nutrition management to increase muscle mass. Because primary and secondary sarcopenia often coexist in people with disability, the concept of rehabilitation nutrition is useful for their treatment. Stroke, hip fracture, and hospital-associated deconditioning are major causes of disability, and inpatients of rehabilitation facilities often have malnutrition and sarcopenia. We review the concept of rehabilitation nutrition, the rehabilitation nutrition options for stroke, hip fracture, hospital-associated deconditioning, sarcopenic dysphagia, and then evaluate the amount of research interest in rehabilitation nutrition.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
