

Tacrine sinusoidal uptake and biliary excretion in sandwich-cultured primary rat hepatocytes
- PMID: 25224352
- PMCID: PMC7928264
- DOI: 10.18433/j3801t
Tacrine sinusoidal uptake and biliary excretion in sandwich-cultured primary rat hepatocytes
Abstract
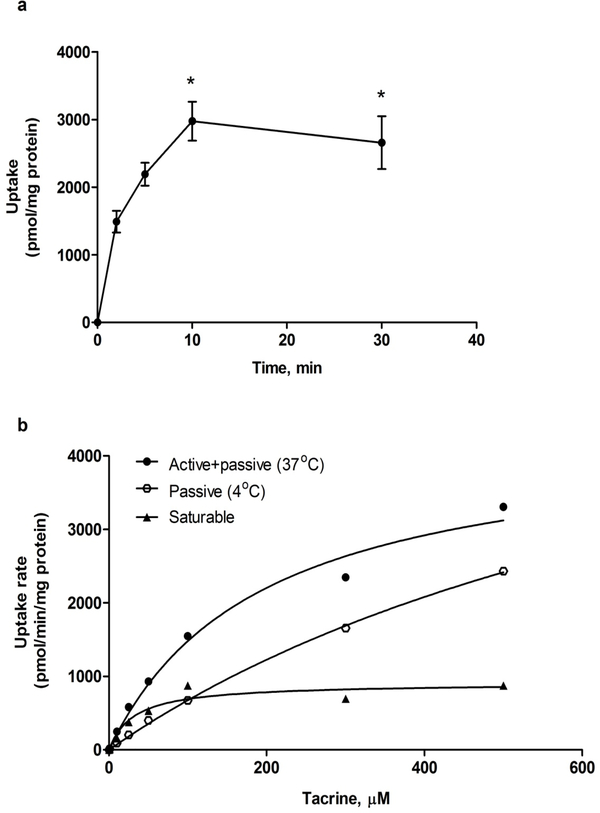
PURPOSE. The knowledge of hepatic disposition kinetics of tacrine, a first cholinesterase inhibitor was approved by FDA for the treatment of Alzheimer's disease (AD), would help to understand its hepatotoxicity, its therapeutic effect, and improve the management of patients with AD. The current study aims to characterize tacrine hepatic transport kinetics and study the role of organic cation transporters (OCTs), P-glycoprotein (P-gp) and multidrug resistance-associated protein (MRP2) in tacrine sinusoidal uptake and biliary excretion. METHODS. Modulation of tacrine hepatic uptake and efflux, biliary excretion index (BEI%), were performed in sandwich-cultured primary rat hepatocytes (SCHs) using transporters inhibitors. Conformation of the integrity of SCHs model was established by capturing images with light-contrast and fluorescence microscopy. RESULTS. Tacrine uptake in SCHs was carrier-mediated process and saturable with apparent Km of 31.5±9.6 µM and Vmax of 908±72 pmol/min/mg protein. Tetraethyl ammonium (TEA), cimetidine and verapamil significantly reduced tacrine uptake with more pronounced effect observed with verapamil which caused 3-fold reduction in tacrine uptake, indicating role for OCTs. Tacrine has a biliary excretion in SCHs with maximum BEI% value of 22.9±1.9% at 10 min of incubation. Addition of MK571 and valspodar decreased the BEI% of tacrine by 40 and 60% suggesting roles for canalicular MRP2 and P-gp, respectively. CONCLUSIONS. Our results show that in addition to metabolism, tacrine hepatic disposition is carrier-mediated process mediated by sinusoidal OCTs, and canalicular MRP2 and P-gp.
Figures





Similar articles
-
In vitro investigation of amyloid-β hepatobiliary disposition in sandwich-cultured primary rat hepatocytes.Drug Metab Dispos. 2013 Oct;41(10):1787-96. doi: 10.1124/dmd.113.052514. Epub 2013 Jul 12. Drug Metab Dispos. 2013. PMID: 23852717
-
Assessment of drug interactions in hepatobiliary transport using rhodamine 123 in sandwich-cultured rat hepatocytes.Drug Metab Dispos. 2005 Mar;33(3):388-94. doi: 10.1124/dmd.104.001669. Epub 2004 Dec 17. Drug Metab Dispos. 2005. PMID: 15608134
-
Species differences in sinusoidal and canalicular efflux transport of mycophenolic acid 7-O-glucuronide in sandwich-cultured hepatocytes.Pharmacol Res Perspect. 2014 Apr;2(2):e00035. doi: 10.1002/prp2.35. Epub 2014 Mar 24. Pharmacol Res Perspect. 2014. PMID: 25505584 Free PMC article.
-
An experimental approach to evaluate the impact of impaired transport function on hepatobiliary drug disposition using Mrp2-deficient TR- rat sandwich-cultured hepatocytes in combination with Bcrp knockdown.Mol Pharm. 2014 Mar 3;11(3):766-75. doi: 10.1021/mp400471e. Epub 2014 Jan 30. Mol Pharm. 2014. PMID: 24410402 Free PMC article.
-
[Evaluation of P-glycoprotein mediated in vitro loperamide biliary excretion with sandwich-cultured rat hepatocytes model].Yao Xue Xue Bao. 2012 Apr;47(4):459-65. Yao Xue Xue Bao. 2012. PMID: 22799027 Chinese.
Cited by
-
Sandwich-Cultured Hepatocytes as a Tool to Study Drug Disposition and Drug-Induced Liver Injury.J Pharm Sci. 2016 Feb;105(2):443-459. doi: 10.1016/j.xphs.2015.11.008. J Pharm Sci. 2016. PMID: 26869411 Free PMC article. Review.
References
-
- Wilkinson DG, Francis PT, Schwam E, Payne-Parrish J. Cholinesterase inhibitors used in the treatment of Alzheimer’s disease: the relationship between pharmacological effects and clinical efficacy. Drugs Aging, 2004; 21(7):453–78. - PubMed
-
- Crismon ML. Tacrine: first drug approved for Alzheimer’s disease. Ann Pharmacother, 1994; 28(6):744–51. - PubMed
-
- Farlow M, Gracon SI, Hershey LA, Lewis KW, Sadowsky CH, Dolan-Ureno J. A controlled trial of tacrine in Alzheimer’s disease. The Tacrine Study Group. JAMA, 1992; 268(18):2523–9. - PubMed
-
- Korabecny J, Spilovska K, Benek O, Musilek K, Soukup O, Kuca K. [Tacrine and its derivatives in the therapy of Alzheimers disease]. Ceska Slov Farm, 2012; 61(5):210–21. - PubMed
-
- Arrieta JL, Artalejo FR. Methodology, results and quality of clinical trials of tacrine in the treatment of Alzheimer’s disease: a systematic review of the literature. Age Ageing, 1998; 27(2):161–79. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous