

TET2 mutations predict response to hypomethylating agents in myelodysplastic syndrome patients
- PMID: 25224413
- PMCID: PMC4208285
- DOI: 10.1182/blood-2014-06-582809
TET2 mutations predict response to hypomethylating agents in myelodysplastic syndrome patients
Abstract
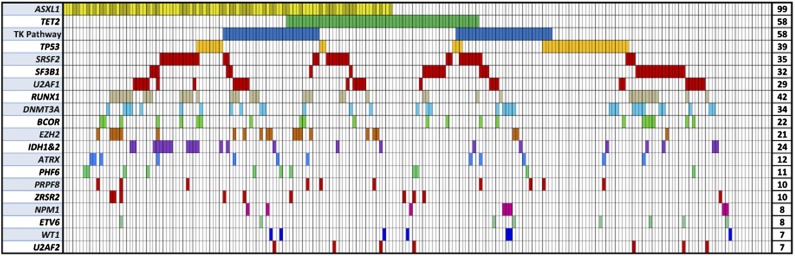
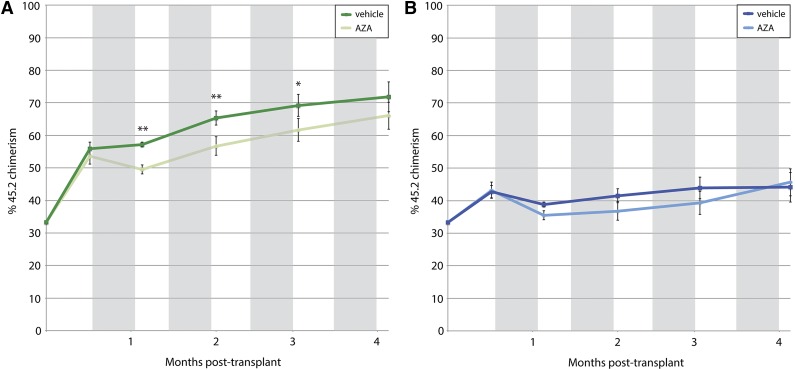
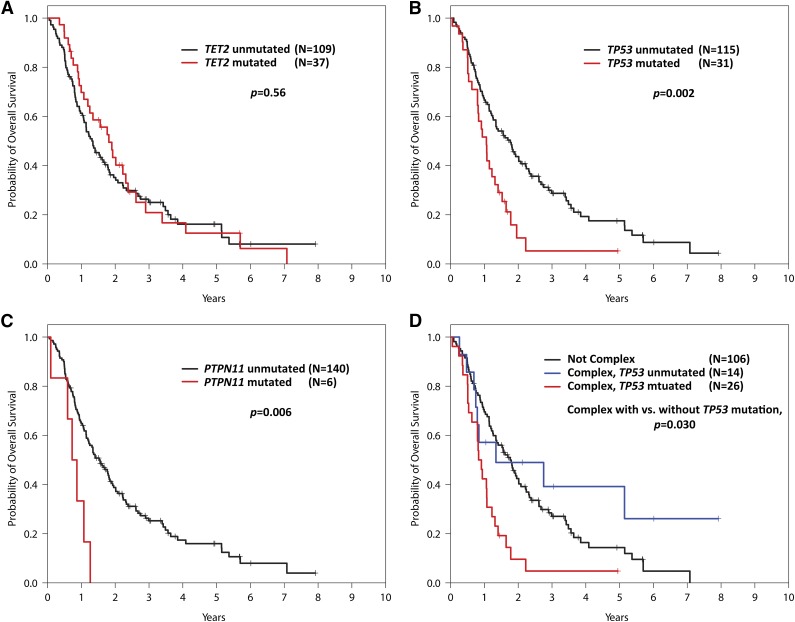
Only a minority of myelodysplastic syndrome (MDS) patients respond to hypomethylating agents (HMAs), but strong predictors of response are unknown. We sequenced 40 recurrently mutated myeloid malignancy genes in tumor DNA from 213 MDS patients collected before treatment with azacitidine (AZA) or decitabine (DEC). Mutations were examined for association with response and overall survival. The overall response rate of 47% was not different between agents. Clonal TET2 mutations predicted response (odds ratio [OR] 1.99, P = .036) when subclones unlikely to be detected by Sanger sequencing (allele fraction <10%) were treated as wild-type (WT). Response rates were highest in the subset of TET2 mutant patients without clonal ASXL1 mutations (OR 3.65, P = .009). Mutations of TP53 (hazard ratio [HR] 2.01, P = .002) and PTPN11 (HR 3.26, P = .006) were associated with shorter overall survival but not drug response. Murine-competitive bone marrow transplantation followed by treatment with AZA demonstrated that Tet2-null cells have an engraftment advantage over Tet2-WT cells. AZA significantly decreased this advantage for Tet2-null cells (P = .002) but not Tet2-WT cells (P = .212). Overall, Tet2 loss appears to sensitize cells to treatment with AZA in vivo, and TET2 mutations can identify patients more likely to respond to HMAs.
© 2014 by The American Society of Hematology.
Figures

Comment in
-
Genome sequencing in myelodysplastic syndromes: can molecular mutations predict benefit from hypomethylating agent therapy?Expert Rev Hematol. 2015 Apr;8(2):155-8. doi: 10.1586/17474086.2015.1016905. Epub 2015 Feb 19. Expert Rev Hematol. 2015. PMID: 25697572
References
-
- Fenaux P, Mufti GJ, Hellstrom-Lindberg E, et al. International Vidaza High-Risk MDS Survival Study Group. Efficacy of azacitidine compared with that of conventional care regimens in the treatment of higher-risk myelodysplastic syndromes: a randomised, open-label, phase III study. Lancet Oncol. 2009;10(3):223–232. - PMC - PubMed
-
- Fenaux P, Ades L. Review of azacitidine trials in Intermediate-2-and High-risk myelodysplastic syndromes. Leuk Res. 2009;33(Suppl 2):S7–S11. - PubMed
-
- Itzykson R, Thépot S, Quesnel B, et al. Groupe Francophone des Myelodysplasies(GFM) Prognostic factors for response and overall survival in 282 patients with higher-risk myelodysplastic syndromes treated with azacitidine. Blood. 2011;117(2):403–411. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
