

Asymptomatic HIV-infected individuals on antiretroviral therapy exhibit impaired lung CD4(+) T-cell responses to mycobacteria
- PMID: 25225948
- PMCID: PMC4299580
- DOI: 10.1164/rccm.201405-0864OC
Asymptomatic HIV-infected individuals on antiretroviral therapy exhibit impaired lung CD4(+) T-cell responses to mycobacteria
Abstract
Rationale: HIV-infected persons on antiretroviral therapy (ART) remain at higher risk of pulmonary tuberculosis (TB) than HIV-uninfected individuals. This increased susceptibility may be caused by impairment of alveolar macrophage (AM) function and/or mycobacteria-specific alveolar CD4(+) T-cell responses observed in HIV-infected ART-naive adults.
Objectives: To determine whether ART was associated with improvement in both AM function, assessed by phagosomal proteolysis, and alveolar CD4(+) T-cell responses to Mycobacterium in HIV-infected individuals.
Methods: Peripheral blood was drawn and bronchoalveolar lavage (BAL) performed on healthy, 35 HIV-uninfected, 25 HIV-infected ART-naive, and 50 HIV-infected ART-treated asymptomatic adults. Phagosomal proteolysis of AM was assessed with fluorogenic beads. Mycobacteria-specific CD4(+) T-cell responses were measured by intracellular cytokine staining.
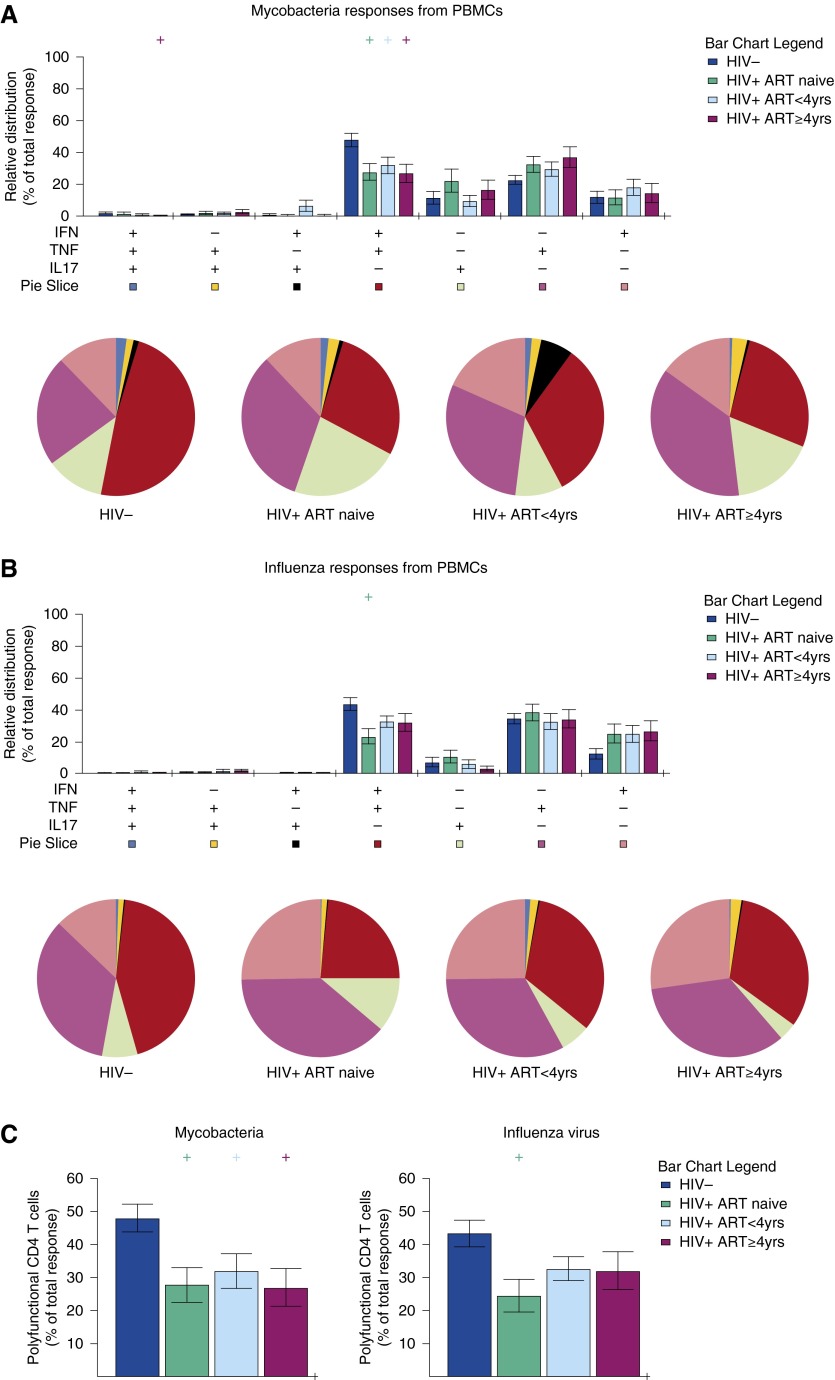
Measurements and main results: HIV-infected adults on ART exhibited lower plasma HIV viral load and higher blood CD4(+) T-cell count than ART-naive adults. AM proteolysis and total mycobacteria-specific Th1 CD4(+) T-cell responses in individuals on ART for greater than or equal to 4 years were similar to HIV-uninfected control subjects but those on ART for less than 4 years had impaired responses. Total influenza-specific alveolar Th1 CD4(+) T-cell responses were intact in all individuals receiving ART. In contrast, BAL and blood mycobacteria-specific polyfunctional CD4(+) T-cell responses were impaired in adults on ART irrespective of duration.
Conclusions: AM and mycobacteria-specific alveolar CD4(+) T-cell responses in HIV-infected adults on ART for less than 4 years are impaired and may partly explain the high risk of TB in HIV-infected individuals on ART. Strategies to augment ART to improve lung immune cell function and reduce the high incidence of TB in HIV-infected adults who initiate ART should be investigated.
Keywords: ART; HIV; Mycobacterium tuberculosis; T cells; macrophages.
Figures




References
-
- Harries AD, Zachariah R, Corbett EL, Lawn SD, Santos-Filho ET, Chimzizi R, Harrington M, Maher D, Williams BG, De Cock KM. The HIV-associated tuberculosis epidemic—when will we act? Lancet. 2010;375:1906–1919. - PubMed
-
- Sonnenberg P, Glynn JR, Fielding K, Murray J, Godfrey-Faussett P, Shearer S. How soon after infection with HIV does the risk of tuberculosis start to increase? A retrospective cohort study in South African gold miners. J Infect Dis. 2005;191:150–158. - PubMed
-
- Houben RM, Crampin AC, Ndhlovu R, Sonnenberg P, Godfrey-Faussett P, Haas WH, Engelmann G, Lombard CJ, Wilkinson D, Bruchfeld J, et al. Human immunodeficiency virus associated tuberculosis more often due to recent infection than reactivation of latent infection. Int J Tuberc Lung Dis. 2011;15:24–31. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
