

CD4 criteria improves the sensitivity of a clinical algorithm developed to identify viral failure in HIV-positive patients on antiretroviral therapy
- PMID: 25227265
- PMCID: PMC4165719
- DOI: 10.7448/IAS.17.1.19139
CD4 criteria improves the sensitivity of a clinical algorithm developed to identify viral failure in HIV-positive patients on antiretroviral therapy
Abstract
Introduction: Several studies from resource-limited settings have demonstrated that clinical and immunologic criteria are poor predictors of virologic failure, confirming the need for viral load monitoring or at least an algorithm to target viral load testing. We used data from an electronic patient management system to develop an algorithm to identify patients at risk of viral failure using a combination of accessible and inexpensive markers.
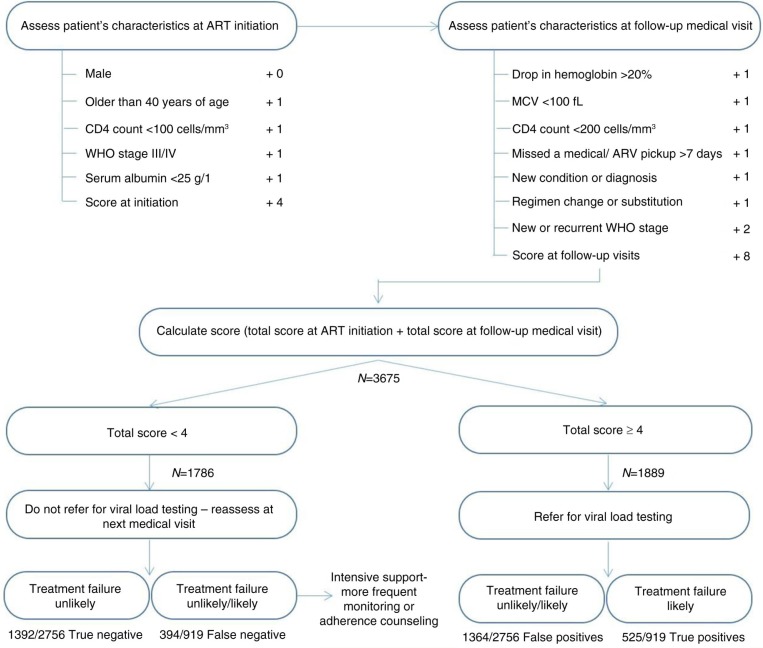
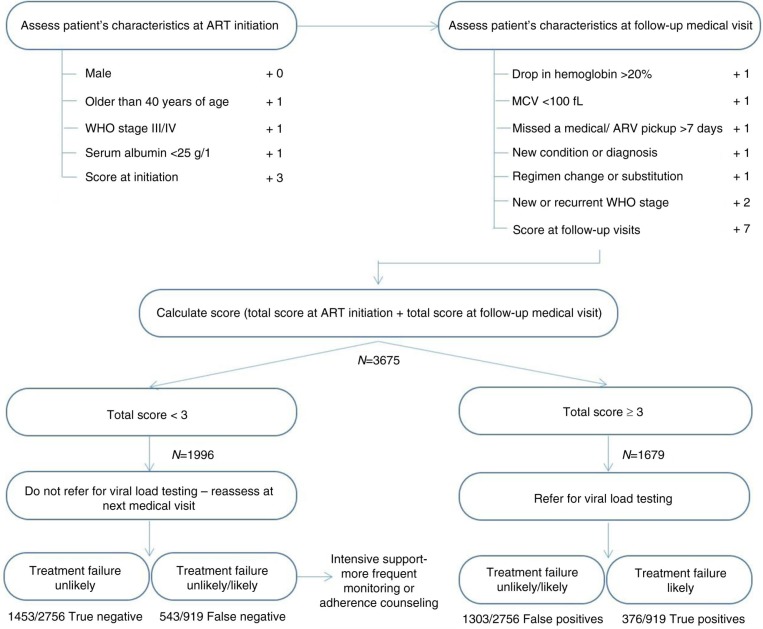
Methods: We analyzed data from HIV-positive adults initiated on antiretroviral therapy (ART) in Johannesburg, South Africa, between April 2004 and February 2010. Viral failure was defined as ≥ 2 consecutive HIV-RNA viral loads >400 copies/ml following suppression ≤ 400 copies/ml. We used Cox-proportional hazards models to calculate hazard ratios (HR) and 95% confidence intervals (CI). Weights for each predictor associated with virologic failure were created as the sum of the natural logarithm of the adjusted HR and dichotomized with the optimal cut-off at the point with the highest sensitivity and specificity (i.e. ≤ 4 vs. >4). We assessed the diagnostic accuracy of predictor scores cut-offs, with and without CD4 criteria (CD4 <100 cells/mm(3); CD4 < baseline; >30% drop in CD4), by calculating the proportion with the outcome and the observed sensitivity, specificity, positive and negative predictive value of the predictor score compared to the gold standard of virologic failure.
Results: We matched 919 patients with virologic failure (1:3) to 2756 patients without. Our predictor score included variables at ART initiation (i.e. gender, age, CD4 count <100 cells/mm(3), WHO stage III/IV and albumin) and laboratory and clinical follow-up data (drop in haemoglobin, mean cell volume (MCV) <100 fl, CD4 count <200 cells/mm(3), new or recurrent WHO stage III/IV condition, diagnosis of new condition or symptom and regimen change). Overall, 51.4% had a score 51.4% had a score ≥ 4 and 48.6% had a score <4. A predictor score including CD4 criteria performed better than a score without CD4 criteria and better than WHO clinico-immunological criteria or WHO clinical staging to predict virologic failure (sensitivity 57.1% vs. 40.9%, 25.2% and 20.9%, respectively).
Conclusions: Predictor scores or risk categories, with CD4 criteria, could be used to identify patients at risk of virologic failure in resource-limited settings so that these patients may be targeted for focused interventions to improve HIV treatment outcomes.
Keywords: CD4; HIV; algorithm; antiretroviral therapy; monitoring; resource limited; viral load.
Figures
Similar articles
-
Immunologic criteria are poor predictors of virologic outcome: implications for HIV treatment monitoring in resource-limited settings.Clin Infect Dis. 2011 Dec;53(12):1283-90. doi: 10.1093/cid/cir729. Clin Infect Dis. 2011. PMID: 22080121 Free PMC article.
-
The role of targeted viral load testing in diagnosing virological failure in children on antiretroviral therapy with immunological failure.Trop Med Int Health. 2012 Nov;17(11):1386-90. doi: 10.1111/j.1365-3156.2012.03073.x. Epub 2012 Sep 14. Trop Med Int Health. 2012. PMID: 22974345 Free PMC article.
-
Long-term virological outcome in children receiving first-line antiretroviral therapy.AIDS Res Ther. 2018 Nov 26;15(1):23. doi: 10.1186/s12981-018-0208-9. AIDS Res Ther. 2018. PMID: 30477526 Free PMC article.
-
Study of the impact of HIV genotypic drug resistance testing on therapy efficacy.Verh K Acad Geneeskd Belg. 2001;63(5):447-73. Verh K Acad Geneeskd Belg. 2001. PMID: 11813503 Review.
-
The future role of CD4 cell count for monitoring antiretroviral therapy.Lancet Infect Dis. 2015 Feb;15(2):241-7. doi: 10.1016/S1473-3099(14)70896-5. Epub 2014 Nov 19. Lancet Infect Dis. 2015. PMID: 25467647 Review.
Cited by
-
Prevalence of antiretroviral therapy treatment failure among HIV-infected pregnant women at first antenatal care: PMTCT Option B+ in Malawi.PLoS One. 2018 Dec 13;13(12):e0209052. doi: 10.1371/journal.pone.0209052. eCollection 2018. PLoS One. 2018. PMID: 30543685 Free PMC article.
-
Interferon-γ-Inducible Protein 10 (IP-10) Kinetics after Antiretroviral Treatment Initiation in Ethiopian Adults with HIV.Microbiol Spectr. 2021 Dec 22;9(3):e0181021. doi: 10.1128/Spectrum.01810-21. Epub 2021 Dec 15. Microbiol Spectr. 2021. PMID: 34908450 Free PMC article.
-
Who Has Yet to Test? A Risk Score for Predicting Never Having Tested for Human Immunodeficiency Virus Among Women and Men in Rural Malawi.Sex Transm Dis. 2019 Jun;46(6):416-421. doi: 10.1097/OLQ.0000000000000989. Sex Transm Dis. 2019. PMID: 31095104 Free PMC article.
-
Clinical predictor score to identify patients at risk of poor viral load suppression at six months on antiretroviral therapy: results from a prospective cohort study in Johannesburg, South Africa.Clin Epidemiol. 2019 May 7;11:359-373. doi: 10.2147/CLEP.S197741. eCollection 2019. Clin Epidemiol. 2019. PMID: 31191029 Free PMC article.
-
Development of an algorithm for determination of the likelihood of virological failure in HIV-positive adults receiving antiretroviral therapy in decentralized care.Glob Health Action. 2017;10(1):1371961. doi: 10.1080/16549716.2017.1371961. Glob Health Action. 2017. PMID: 28914169 Free PMC article.
References
-
- Joint United Nations Programme on HIV/AIDS (UNAIDS) Global report: UNAIDS report on the global AIDS epidemic 2013. ISBN 978-92-9253-032-7 [Internet]. [cited 2014 Feb 7]. Available from: http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiolo....
-
- Zachariah R, Fitzgerald M, Massaquoi M, Pasulani O, Arnould L, Makombe S, et al. Risk factors for high early mortality in patients on antiretroviral treatment in a rural district of Malawi. AIDS. 2006;20:2355–60. - PubMed
-
- Mellors J, Muñoz A, Giorgi J, Margolick JB, Tassoni CJ, Gupta P, et al. Plasma viral load and CD4+ lymphocytes as prognostic markers of HIV-1 infection. Ann Intern Med. 1997;126:946–54. - PubMed
-
- Lynen L, An S, Koole O, Thai S, Ros S, De Munter P, et al. An algorithm to optimize viral load testing in HIV-positive patients with suspected first-line antiretroviral therapy failure in Cambodia. J Acquir Immune Defic Syndr. 2009;52(1):40–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
