

Impact of chronic kidney disease on the prevalence of cardiovascular disease in patients with type 2 diabetes in Spain: PERCEDIME2 study
- PMID: 25227555
- PMCID: PMC4181296
- DOI: 10.1186/1471-2369-15-150
Impact of chronic kidney disease on the prevalence of cardiovascular disease in patients with type 2 diabetes in Spain: PERCEDIME2 study
Abstract
Background: The presence of chronic kidney disease (CKD) in type 2 diabetes mellitus (T2DM) increases the risk of cardiovascular disease (CVD) regardless of the presence of traditional cardiovascular risk factors. There is controversy about the impact of each of the manifestations of CKD on the prevalence of CVD, whether it is greater with decreased estimated glomerular filtration rate (eGFR) or increased urine albumin creatinine ratio (UACR).
Methods: This study is a national cross-sectional study performed in primary care consults. We selected participants of both sexes who were aged 40 years or older, had been diagnosed with T2DM and had complete information on the study variables recorded in their medical records. The participants were classified according to eGFR : ≥ 60; 45-59; 30-44; <30 mL/min/1.73 m(2) and UACR : < 30; 30-299; ≥ 300 mg/gr. The results were adjusted to compare the prevalence of CVD across all categories.
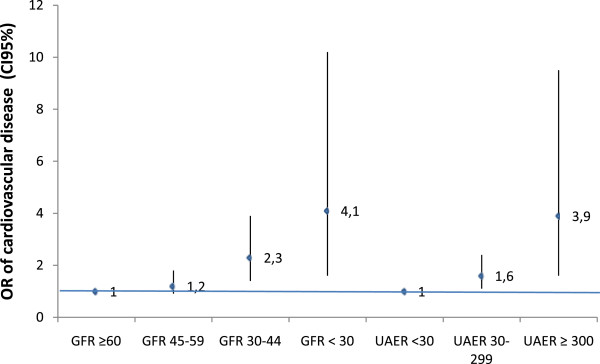
Results: A total of 1141 participants were included. Compared to participants with eGFR > 60 mL/min/1.73 m(2) those with eGFR between 30-44 mL/min/m(2), (OR = 2.3; 95% CI, 1.4-3.9); and eGFR < 30 mL/min/1.73 m(2) (OR = 4.1 95% CI 1.6-10.2) showed increased likelihood of having CVD. Participants with UACR ≥ 30 mg/g compared to participants with UACR < 30 mg/g increased significantly the likelihood of having CVD, especially with UACR above 300 mg/g, (OR = 1.6; 95% CI 1.1-2.4 for UACR = 30-299 mg/g; OR = 3.9; CI 1.6-9.5 for UACR ≥ 300 mg/g).
Conclusion: The decrease in eGFR and increase in UACR are independent risk factors that increase the prevalence of CVD in participants with T2DM and these factors are independent of each other and of other known cardiovascular risk factors. In our study the impact of mild decreased eGFR in T2DM on CVD was lower than the impact of increased UACR. It is necessary to determine not only UACR but also eGFR for all patients with T2DM, both at the time of diagnosis and during follow-up, to identify those patients at high risk of cardiovascular complications.
Figures
References
-
- Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, McCullough PA, Kasiske BL, Kelepouris E, Klag MJ, Parfrey P, Pfeffer M, Raij L, Spinosa DJ, Wilson PW, American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation. 2003;108:2154–2169. doi: 10.1161/01.CIR.0000095676.90936.80. - DOI - PubMed
-
- Levey AS, Atkins R, Coresh J, Cohen EP, Collins AJ, Eckardt KU, Nahas ME, Jaber BL, Jadoul M, Levin A, Powe NR, Rossert J, Wheeler DC, Lameire N, Eknoyan G. Chronic kidney disease as a global public health problem: approaches and initiatives a position statement from Kidney Disease Improving Global Outcomes. Kidney Int. 2007;72:247–259. doi: 10.1038/sj.ki.5002343. - DOI - PubMed
-
- Fox CS, Matsushita K, Woodward M, Bilo HJ, Chalmers J, Heerspink HJ, Lee BJ, Perkins RM, Rossing P, Sairenchi T, Tonelli M, Vassalotti JA, Yamagishi K, Coresh J, de Jong PE, Wen CP, Nelson RG, Chronic Kidney Disease Prognosis Consortium Chronic Kidney Disease Prognosis Consortium. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: a meta-analysis. Lancet. 2012;380:1662–1673. doi: 10.1016/S0140-6736(12)61350-6. - DOI - PMC - PubMed
Pre-publication history
-
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2369/15/150/prepub
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
