

A prospective study comparing infection risk and disease activity in children with juvenile idiopathic arthritis treated with and without tumor necrosis factor-alpha inhibitors
- PMID: 25227771
- PMCID: PMC4351171
- DOI: 10.1007/s10067-014-2779-8
A prospective study comparing infection risk and disease activity in children with juvenile idiopathic arthritis treated with and without tumor necrosis factor-alpha inhibitors
Abstract
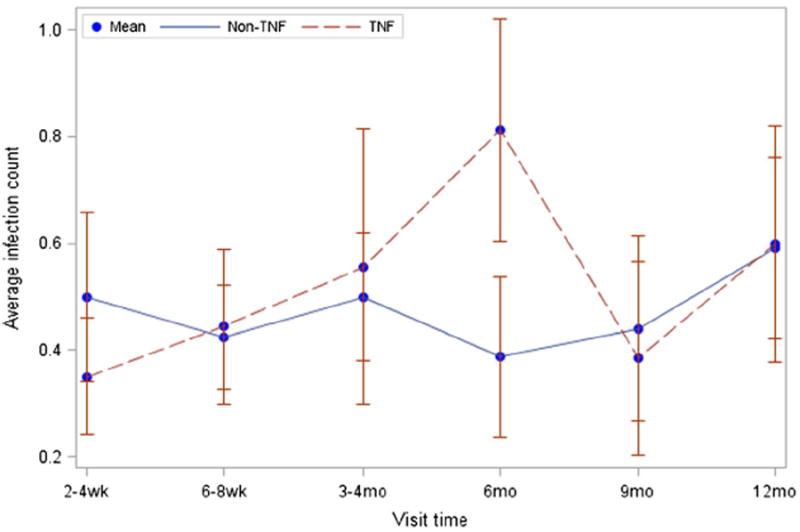
Tumor necrosis factor-alpha (TNF-α) inhibitors are effective treatment for juvenile idiopathic arthritis (JIA) but may increase infection rates. However, active JIA may also render patients vulnerable to infection. In this study, we prospectively assessed infection rates in JIA patients treated with and without TNF-α inhibitors and correlated disease activity with infection risk. TNF-α inhibitor-naïve JIA subjects were followed up for 12 months. Subjects initiated on TNF-α inhibitors after enrollment were analyzed in the TNF group. Subjects treated without TNF-α inhibitors were analyzed in the non-TNF group. Questionnaires captured mild or severe infections. JIA disease activity by Childhood Health Assessment Questionnaire (CHAQ) disability index/pain score and physician joint count/global assessment was recorded. Twenty TNF and 36 non-TNF subjects were analyzed. The total infection rate ratio for TNF versus non-TNF group subjects was 1.14 (95% CI, 0.78-1.66; p = 0.51). The average rate of infections per month was 0.29 for TNF and 0.24 for non-TNF subjects. No severe infections or hospitalizations occurred in either group. Secondary infectious outcomes were also similar between groups. Controlling for study group, an increase in CHAQ pain score correlated with an increase in several infectious outcome measures. Our results suggest no difference in infection rates between JIA subjects treated with and without TNF-α inhibitors. Additionally, JIA disease activity may have contributed to infection risk in our cohort, irrespective of immunosuppressive therapy. Future analysis of the relationship between treatment regimens, disease activity, and infection rates may help to further delineate predictors of infection risk in JIA patients.
Figures
References
-
- Ruperto N, Lovell DJ, Cuttica R, Wilkinson N, Woo P, Espada G, et al. A randomized, placebo-controlled trial of infliximab plus methotrexate for the treatment of polyarticular-course juvenile rheumatoid arthritis. Arthritis Rheum. 2007;56:3096–3106. - PubMed
-
- Gerloni V, Pontikaki I, Gattinara M, Fantini F. Focus on adverse events of tumour necrosis factor alpha blockade in juvenile idiopathic arthritis in an open monocentric long-term prospective study of 163 patients. Ann Rheum Dis. 2008;67:1145–1152. - PubMed
-
- Lovell DJ, Giannini EH, Reiff A, Cawkwell GD, Silverman ED, Nocton JJ, et al. Etanercept in children with polyarticular juvenile rheumatoid arthritis. N Engl J Med. 2000;342:763–769. - PubMed
-
- Lovell DJ, Reiff A, Ilowite NT, Wallace CA, Chon Y, Lin S, et al. Safety and efficacy of up to eight years of continuous etanercept therapy in patients with juvenile rheumatoid arthritis. Arthritis Rheum. 2008;58:1496–1504. - PubMed
-
- Lovell DJ, Ruperto N, Goodman S, Reiff A, Jung L, Jarosova K. Adalimumab with or without methotrexate in juvenile rheumatoid arthritis. N Engl J Med. 2008;359:810–820. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
