

doi: 10.1158/1078-0432.CCR-14-2123.
Epub 2014 Sep 16.
AACR Cancer Progress Report 2014
- PMID: 25228531
- PMCID: PMC4666597
- DOI: 10.1158/1078-0432.CCR-14-2123
Item in Clipboard
AACR Cancer Progress Report 2014
Clin Cancer Res.
.
No abstract available
Conflict of interest statement
No potential conflicts of interest were disclosed by the other authors.
Figures
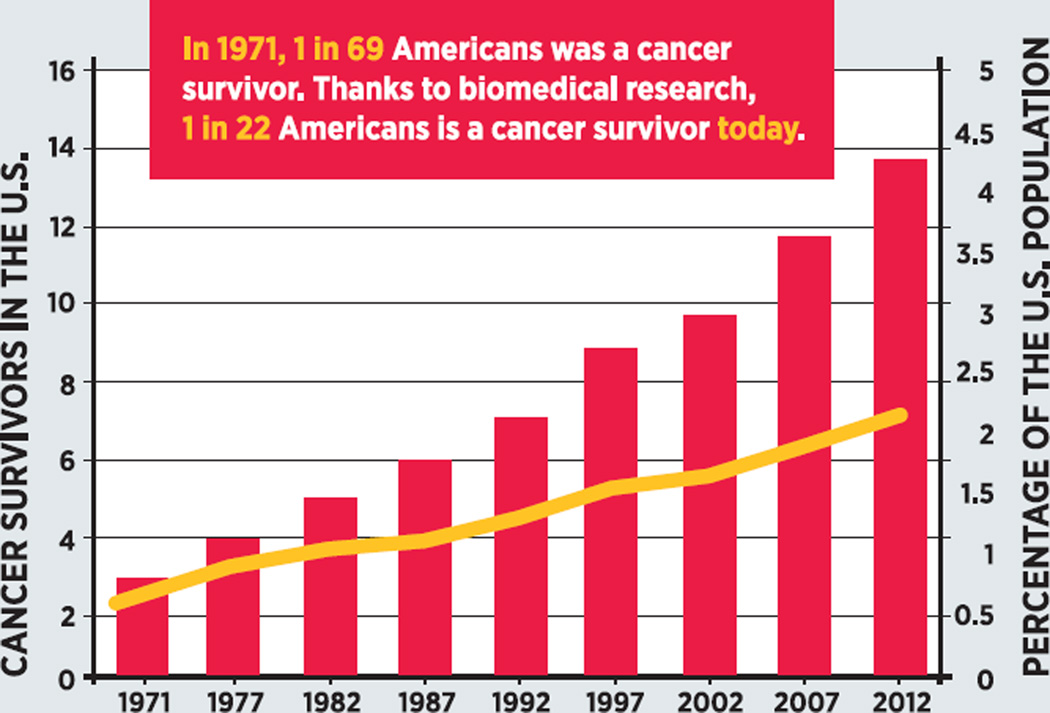
The number of cancer survivors in the United States has steadily increased since 1971 [red bars]. During the same period, the proportion of the nation’s population that is living with, through, or beyond a cancer diagnosis has more than tripled [gold line]. Adapted from (5).
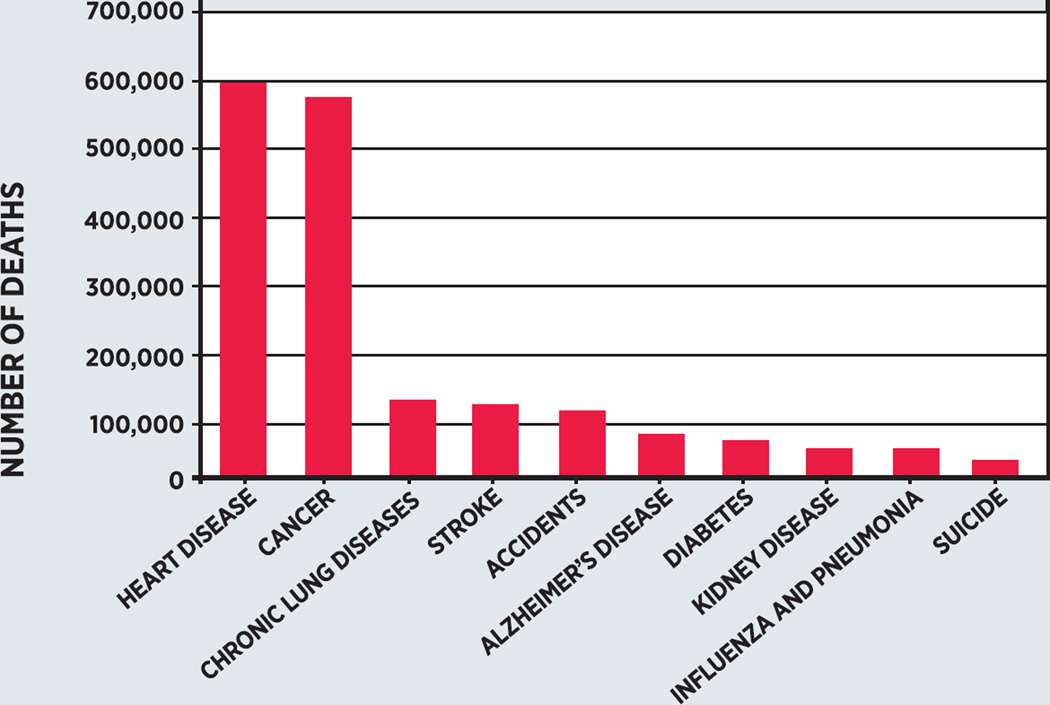
Together, heart disease and cancer caused approximately half of the 2,468,435 deaths that occurred in the United States in 2010. Moreover, each resulted in more than four times the number of deaths as the third most common cause of death, chronic lung diseases. If current trends continue, cancer will soon overtake heart disease as the leading cause of death for all Americans; it has already done so among the U.S. Hispanic population (13). Data from (12).

Many cancers are progressive in nature. In the general example depicted here, normal cells first take on precancerous characteristics. As these cells multiply and evolve, the precancerous lesion becomes a tumor that gradually gets larger and extends to lymph nodes as it becomes more advanced, ultimately metastasizing. Assessing the degree to which a patient’s cancer has progressed helps doctors select an appropriate treatment and estimate prognosis or predict outcome. Staging is the term used to describe the severity of a person’s cancer. Most solid tumors, except for brain and spinal tumors, are staged using the TNM system; gynecological cancers use a variant of the TNM system. The system is based on tumor size (T), reach to local lymph nodes (N), and extent of spread in the body (metastasis; M). Each organ has a specific set of guidelines for determining stage using the TNM system.
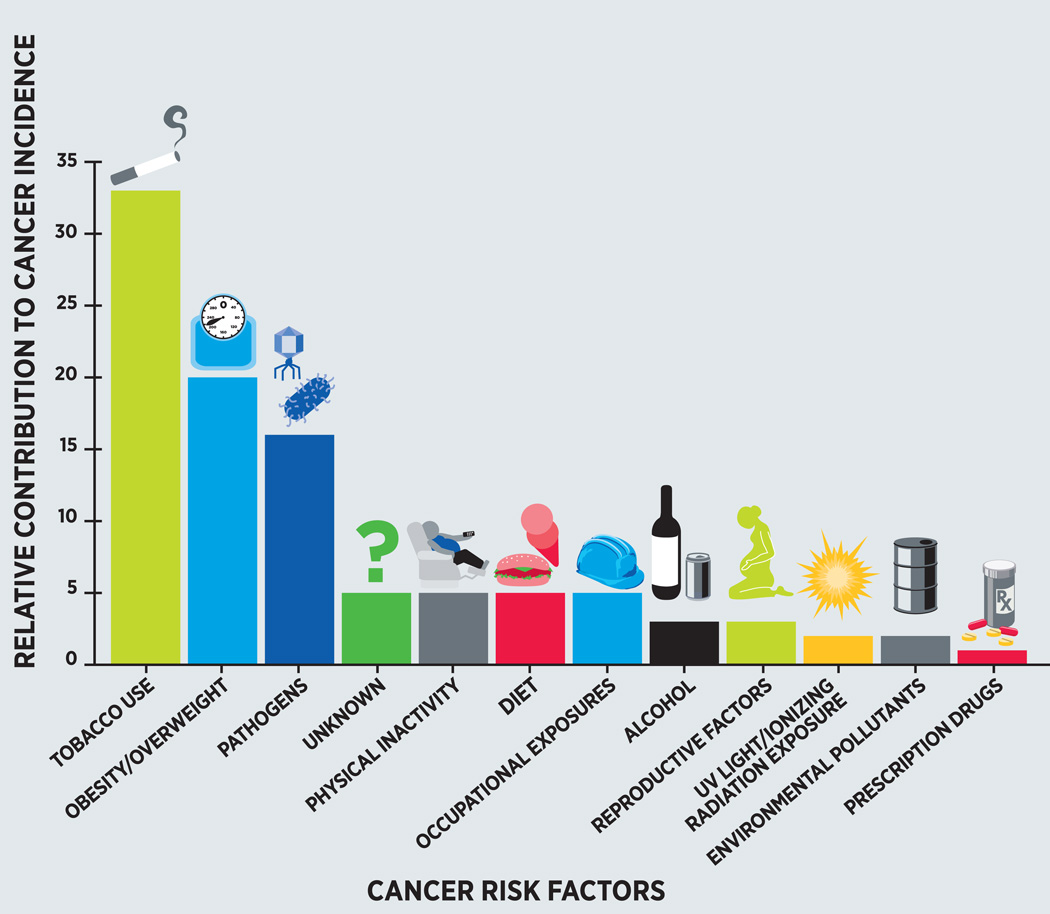
Research has identified numerous factors that increase an individual’s risk for developing cancer. Not all factors have the same impact on cancer risk. The factors with the biggest impact are tobacco use, obesity and overweight, infection with one of several pathogens, lack of physical activity, and poor dietary habits. Adopting healthy approaches to living (see Figure 5) could eliminate or reduce many of these risks and therefore have a tremendous influence on our nation’s burden of cancer. Data from (16); figure adapted from (5).

Research has identified numerous factors that affect a person’s risk of developing cancer (see Figure 4). Many of the factors with the greatest influence on cancer risk can be eliminated or reduced by adopting a healthy approach to living. For example, ending tobacco use, eating a healthy and balanced diet, undertaking regular physical activity, reducing exposure to the sun, managing pre-existing medical conditions with the appropriate medications, getting vaccinated against certain pathogens, and developing a personalized cancer-screening program with a physician (or physicians) are all part of a healthy approach to living.
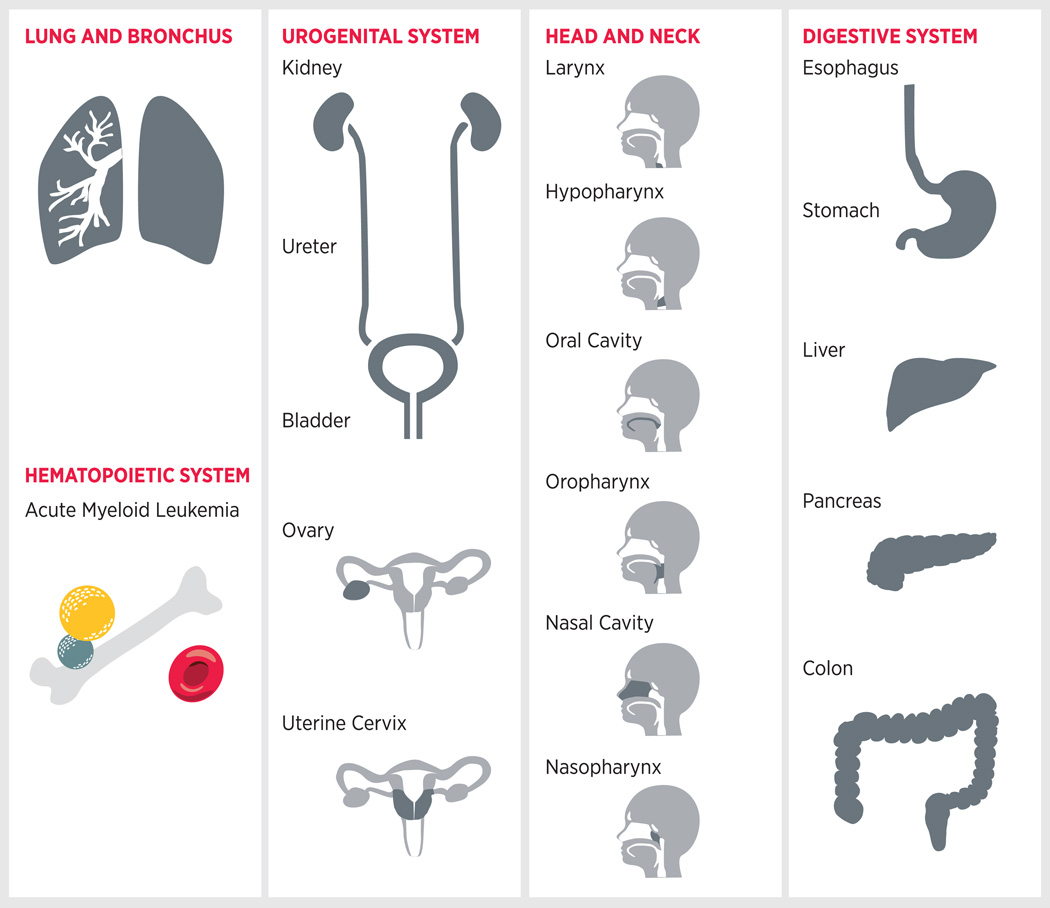
Tobacco use increases an individual’s risk of developing not only lung cancer but also 17 other types of cancer (11). This explains why tobacco use will account for an estimated 30 percent of all cancer deaths in the United States in 2014 (1).
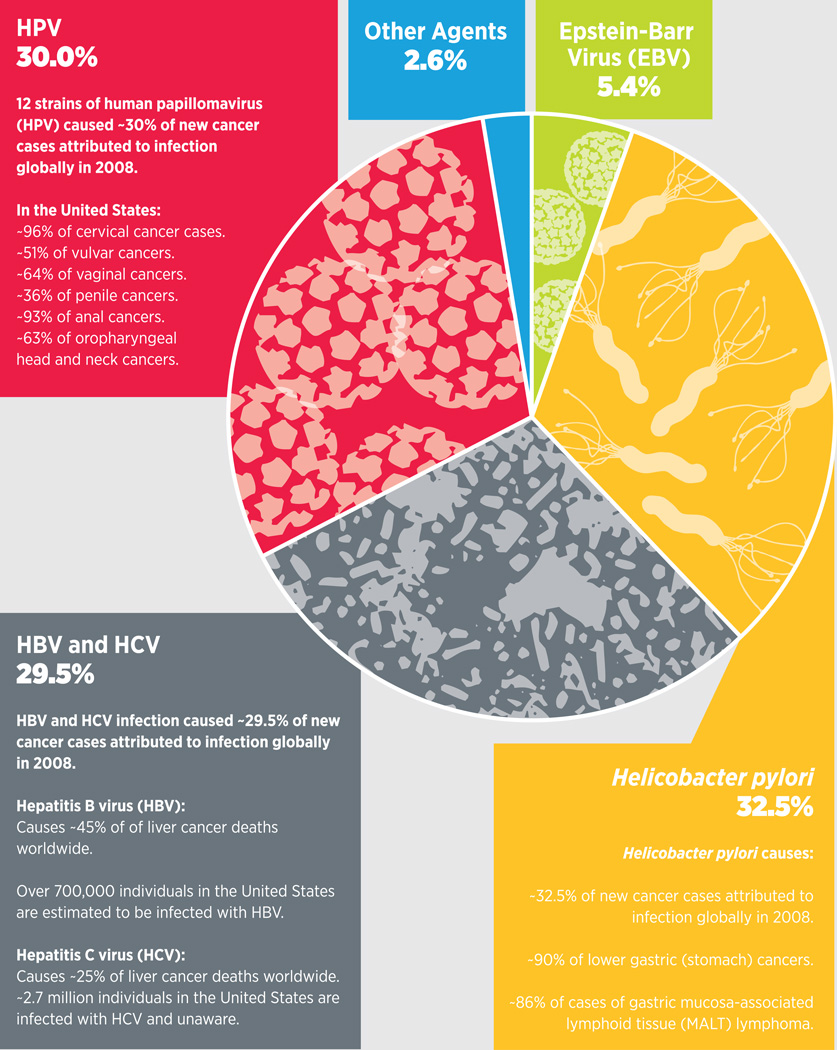
Persistent infection with a number of pathogens is estimated to cause approximately 2 million cases of cancer worldwide each year (42) (see Table 4, p. 22). More than 90 percent of these cases are attributable to just four pathogens—Helicobacter pylori, hepatitis B virus (HBV), hepatitis C virus (HCV), and human papillomavirus (HPV). Each pathogen is linked with a specific type of cancer or cancers, and strategies exist to eliminate or prevent infection with some of these cancer-associated pathogens (see sidebar Cancer-causing Pathogens: Prevention and Elimination, p. 24). It is clear, however, that a dramatic reduction in the global incidence of these types of cancer could be achieved by more effective implementation of such strategies. Data from (–49); figure adapted from (50).
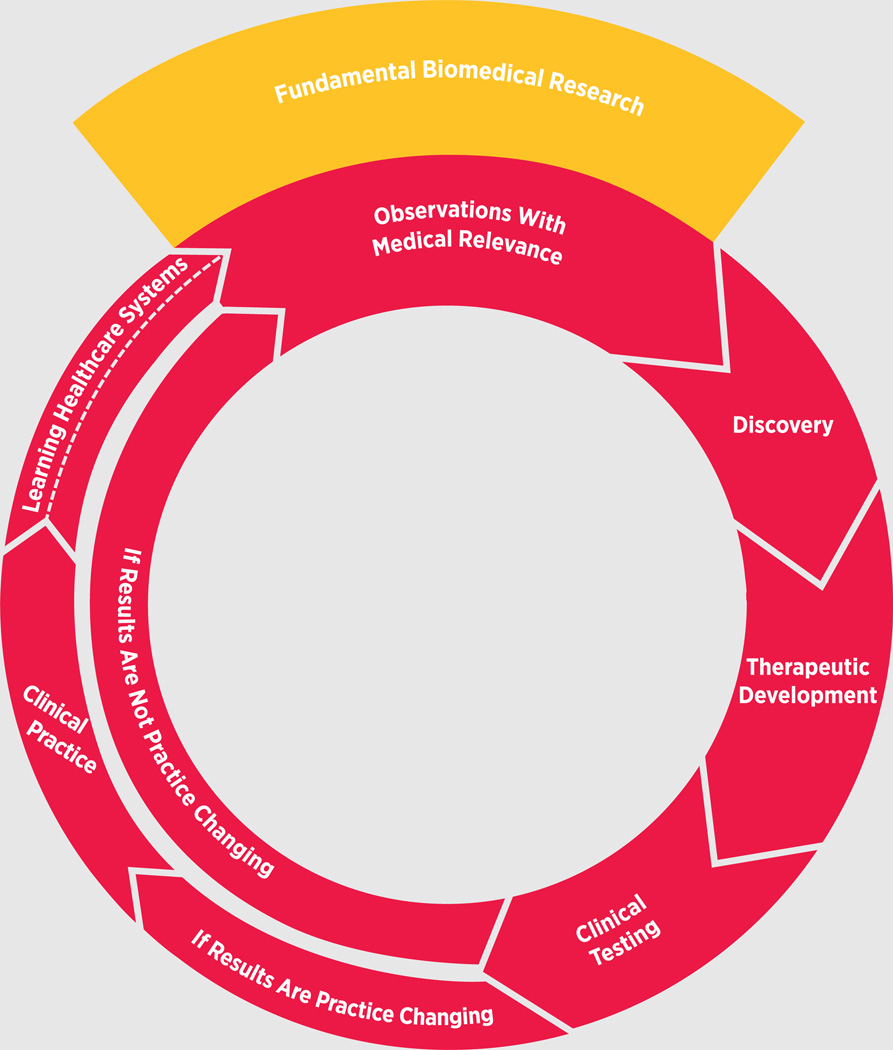
Biomedical research begins with observations relevant to the practice of medicine, which lead to questions, or hypotheses, that are tested in experiments during the discovery phase of research (see sidebars on Who We Are, p. 32, and Research Models, p. 34). During the discovery phase, traits unique to a disease may be uncovered, leading to the development of a potential therapeutic (see sidebar on Therapeutic Development, p. 35). Before entering clinical testing, potential therapeutics are subjected to preclinical testing to identify any toxicities and help with initial dosing. Clinical testing is a multiphase process aimed at demonstrating the safety and efficacy of a potential therapeutic (see sidebar on Phases of Clinical Trials, p. 38). If a therapeutic is safe and effective and is approved for use by the U.S. Food and Drug Administration (FDA), it will enter into clinical practice, where it can transform the lives of patients. Importantly, observations made during the routine use of a new therapeutic can feed back into the biomedical research cycle and further enhance the use of that therapeutic or the development of others like it. If, however, a therapeutic is not safe or effective and fails to gain FDA approval, the observations from the clinical testing can feed back into the biomedical research cycle to spur future research efforts. Because the cycle is iterative, it is constantly building on prior knowledge.

One of the major uses of genomics in clinical research is in the design and execution of novel clinical trials. Two such types of trials are basket and umbrella trials. In the basket trial depicted here, one drug is being tested against a particular genetic mutation (green dots) across liver, lung, bone, colon, and stomach cancers. In the umbrella trial illustrated here, three different drugs are being tested against multiple genetic mutations (yellow, green, blue, and red dots) within lung cancer.
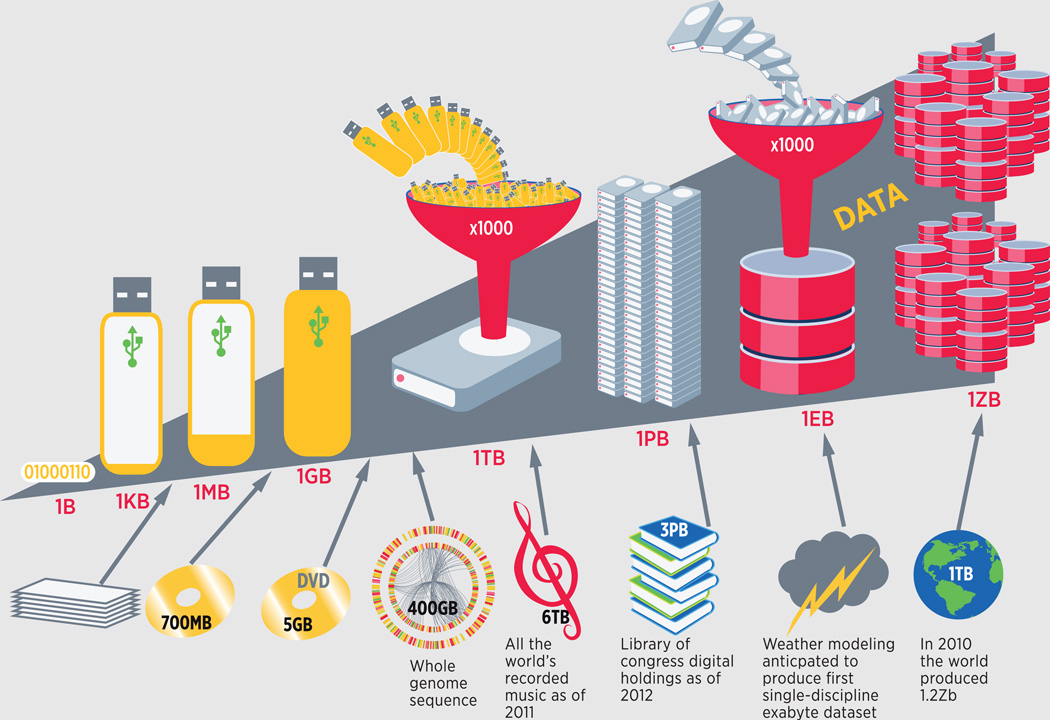
Data of any kind are measured in bytes. A byte (B) is 8 binary digits (the 01011010 below) and is recognized by a computer as a single character. A thousand bytes make up a kilobyte (kB); the average Word document (stack of paper) is tens to hundreds of kB. The average compact disc can hold 700,000 kB, which is 700 megabytes (MB) of data (gold disc). A thousand MB are contained within a gigabyte (GB), illustrated by the thumb drive, and the average digital video disc (DVD) holds nearly 5 GB of data (gold DVD). It would take more than 80 DVDs to store the data from sequencing an individual’s entire genome (the circos plot), which is approximately 400 GB. A 2011 McKinsey Global Institute (MGI) report estimated that all of the world’s recorded music up to that year could be stored in 6 terabytes (TB; music note); it would take 60001-GB thumb drives to store all of this data (73). As of April 25, 2012, the Library of Congress’ digital holdings collection contained 3 petabytes (PB; bookcase) of data, which totals 3000 terabytes or 3 million 1-GB thumb drives (74). Researchers at the Lawrence Berkeley National Laboratory forecast that within the next few years, it will generate more than an exabyte (EB; cloud) of data modeling the weather. It would take more than 1 billion 1-GB thumb drives to store these data (71). It is estimated that in 2010, the world collectively created more than 1.2 zetabytes (ZB; globe) of data (72). Big datasets are unique in that they are too large to be stored and analyzed using traditional methods. The complexity of cancer and its treatment is creating big datasets, and the field and the patients it serves will benefit greatly from research into how to optimize systems for storing, accessing, and analyzing big data.
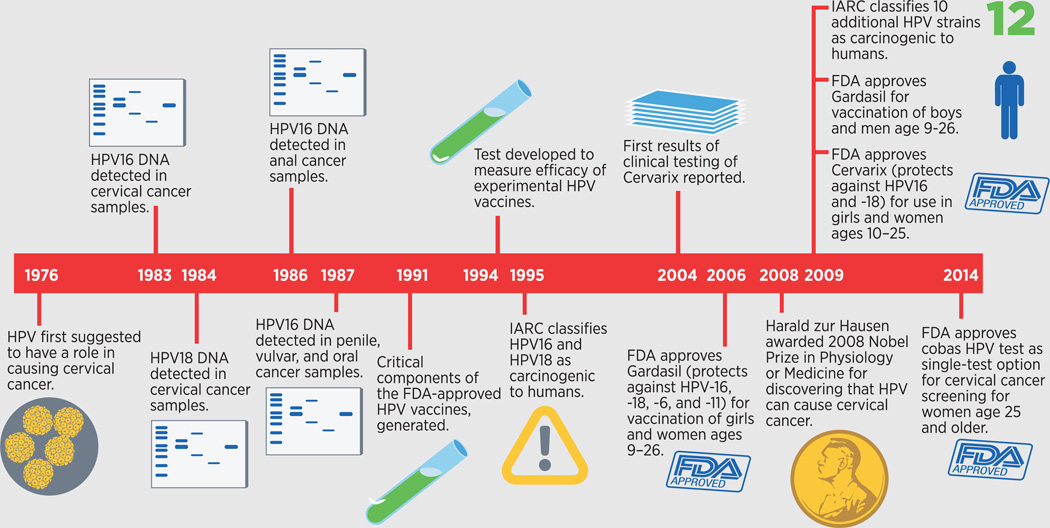
Human papillomavirus (HPV) was first suggested to have an important role in causing cervical cancer in 1976. During the ensuing years, researchers confirmed this hypothesis and identified the cancer-causing strains of HPV. They also found that certain strains of HPV cause many cases of anal, penile, vaginal, and vulvar cancers (see Figure 7, p. 23). Thirty years after the first suggestion of a cancer-causing role for HPV, the dedicated efforts of many basic and clinical researchers across the biomedical research enterprise culminated in approval by the U.S. Food and Drug Administration (FDA) of a vaccine that prevents infection with the two most common cervical cancer-causing HPV strains, HPV16 and HPV18, after the vaccine was shown to prevent precancerous cervical abnormalities caused by these strains. Since then, the FDA has approved a second HPV vaccine and the use of an HPV test called the cobas HPV test as a stand-alone option for cervical cancer screening for women age 25 and older. Research efforts are now focusing on developing vaccines that target more of the cancer-causing HPV strains and implementing effective strategies to increase vaccine usage.
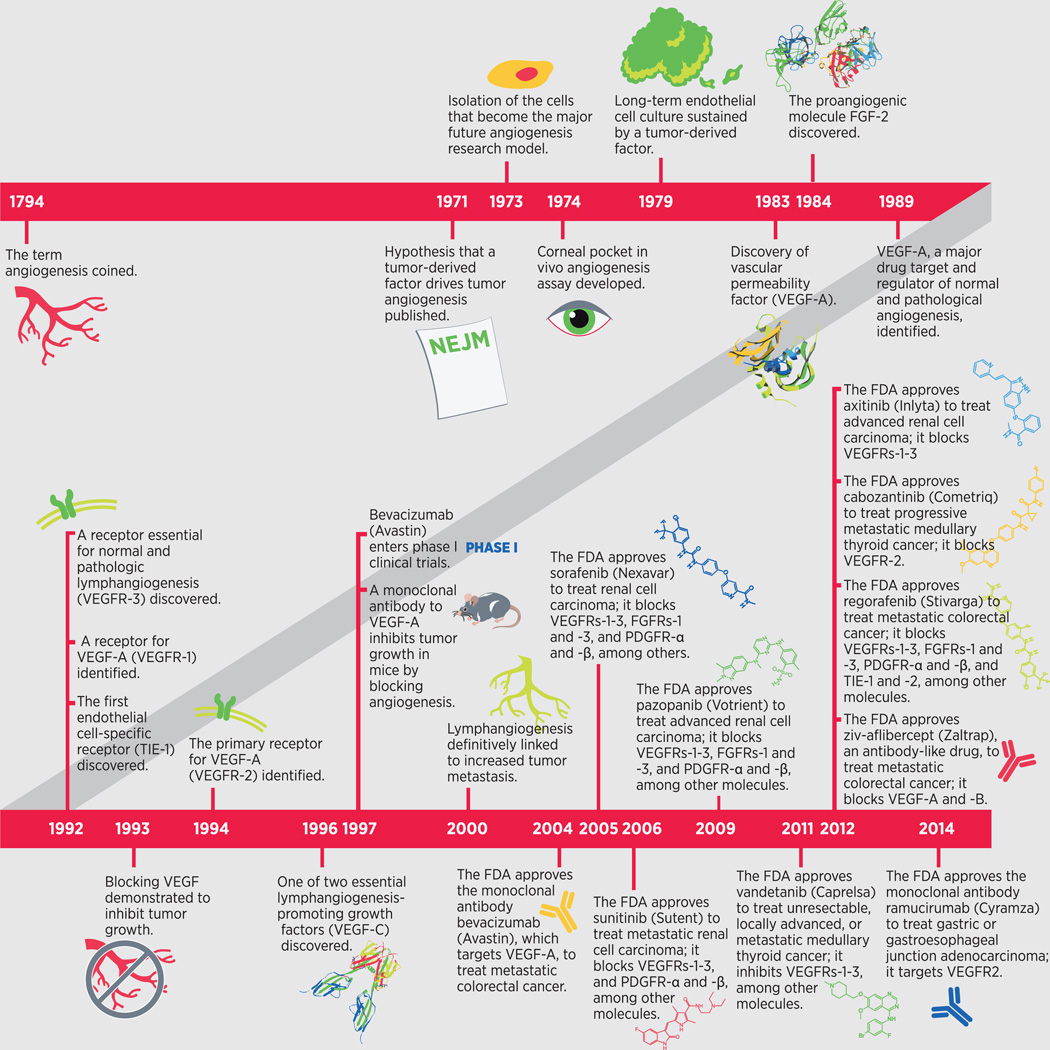
In the past 10 years, the U.S. Food and Drug Administration (FDA) has approved 10 anticancer therapeutics that work by blocking the development of new blood vessels (angiogenesis). Bevacizumab (Avastin) was the first of these drugs, known as antiangiogenic agents, to be approved, in 2004, and ramucirumab (Cyramza) is the most recent, in 2014. Research into the processes of angiogenesis and lymphangiogenesis, in both normal and pathological conditions including cancer, helped identify many of the molecular regulators of these processes, and these regulators are the specific targets of the 10 antiangiogenic agents. The first date of approval for each of these therapeutics is indicated on the timeline; however, most of these agents received approval from the FDA for the treatment of additional cancers in subsequent years. Pathological angiogenesis also underlies neurovascular age-related macular degeneration, a major cause of blindness. Two antiangiogenic agents—ranibizumab (Lucentis), a derivative of bevacizumab (Avastin), and aflibercept (Eylea)—are FDA approved for the treatment of this form of eye disease and may be approved for other forms in the near future. Thus, cancer research can benefit patients with diseases other than cancer.
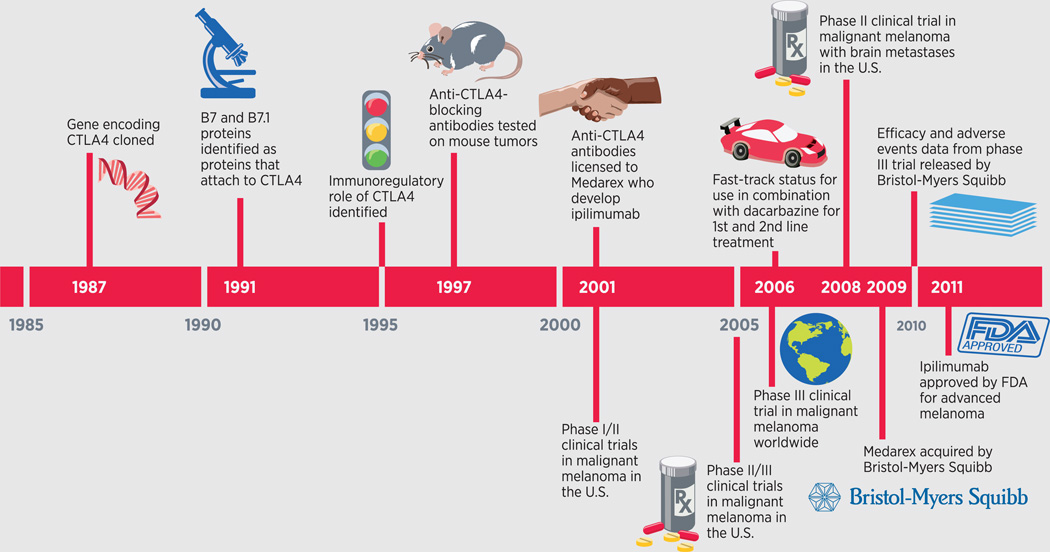
Ipilimumab (Yervoy) is an immunotherapeutic that works by counteracting a brake on cancer-fighting immune cells called CTLA4. It is currently the only drug of its kind to be approved by the U.S. Food and Drug Administration (FDA). Almost 25 years of basic and clinical research underpinned the development of ipilimumab. The story began in 1987, when researchers discovered a gene they called CTLA4. It then took nearly eight years before the function of CTLA4 was uncovered, and another 16 years before this knowledge was translated into ipilimumab. Several other drugs in development target another immune-cell brake called PD1, and others target the tumor protein that steps on this brake, PD-L1. Adapted from (5).
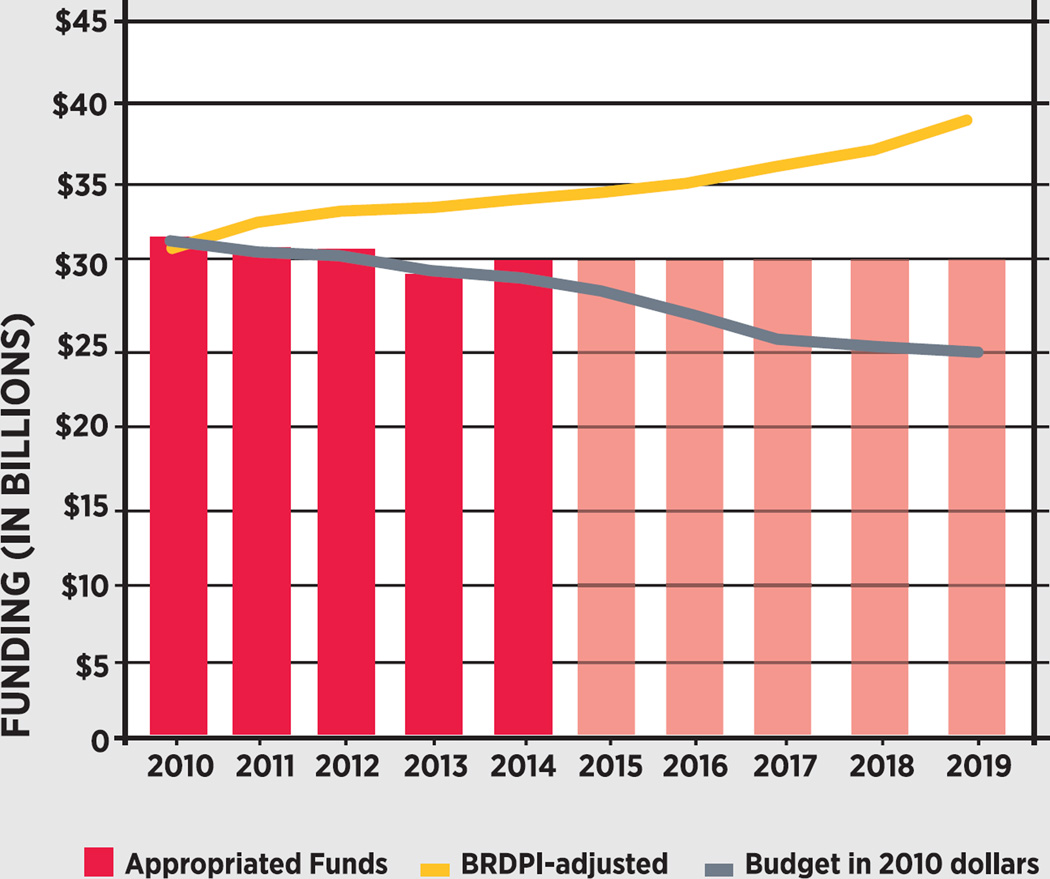
The Biomedical Research and Development Price Index (BRDPI) reflects the rising cost of personnel, supplies, and equipment needed to conduct biomedical research. The red bars indicate National Institutes of Health (NIH) budget levels, and the red transparent bars are an estimated budget based on 2014 levels. The gray line indicates that the current effective funding level for the NIH is $3.5 billion less than where it would have been today if it had simply grown at the same rate as BRDPI since 2010 (gold line). This discrepancy translates into a loss of more than $5 billion in purchasing power. Congress is faced with a choice. It can choose to make biomedical research a priority by funding the NIH at a level at least commensurate with BRDPI (gold line). If it chooses to fund biomedical research at the current rate, the budget of the NIH will continue along the gray line, and patients will undoubtedly be affected. Thus, it is clear that there is only one viable path forward (gold line).
References
-
- American Cancer Society. Cancer facts & figures 2014. Atlanta (GA): ACS; 2014.
-
- Cancer survivorship—United States, 1971–2001. MMWR Morb Mortal Wkly Rep. 2004;53:526–529. - PubMed
-
- American Cancer Society. Cancer treatment and survivorship facts & figures 2014–2015. Atlanta (GA): ACS; 2014.
-
- Howden LM, Meyer JA. Age and sex composition: 2010. Washington, DC: U.S. Department of Commerce Economics and Statistics Administration, U.S. Census Bureau; 2011. [cited 2014 Jul 31]. Available from: http://www.census.gov/prod/cen2010/briefs/c2010br-03.pdf.
-
- Sawyers CL, Abate-Shen C, Anderson KC, Barker A, Baselga J, Berger NA, et al. AACR Cancer progress report 2013. Clin Cancer Res. 2013;19:S4–S98. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
