

Prediction of sarcomere mutations in subclinical hypertrophic cardiomyopathy
- PMID: 25228707
- PMCID: PMC4237712
- DOI: 10.1161/CIRCIMAGING.114.002411
Prediction of sarcomere mutations in subclinical hypertrophic cardiomyopathy
Abstract
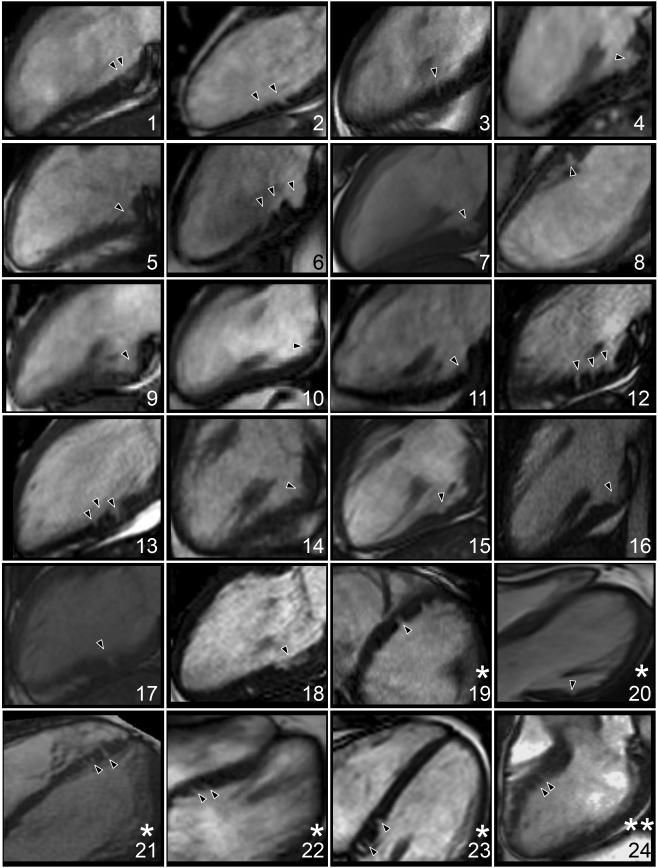
Background: Sarcomere protein mutations in hypertrophic cardiomyopathy induce subtle cardiac structural changes before the development of left ventricular hypertrophy (LVH). We have proposed that myocardial crypts are part of this phenotype and independently associated with the presence of sarcomere gene mutations. We tested this hypothesis in genetic hypertrophic cardiomyopathy pre-LVH (genotype positive, LVH negative [G+LVH-]).
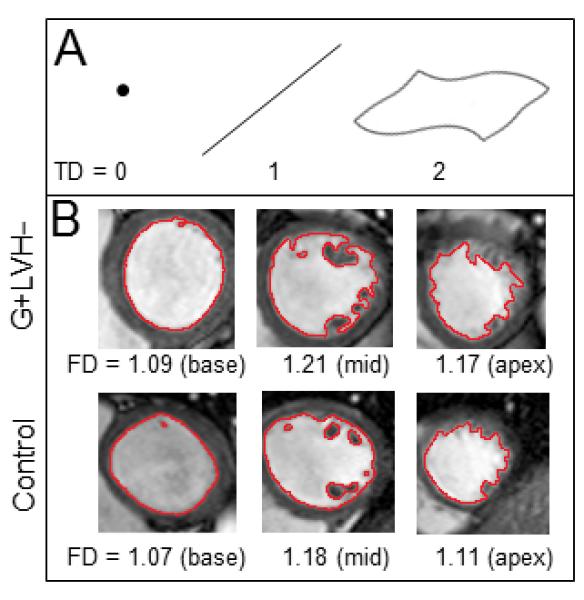
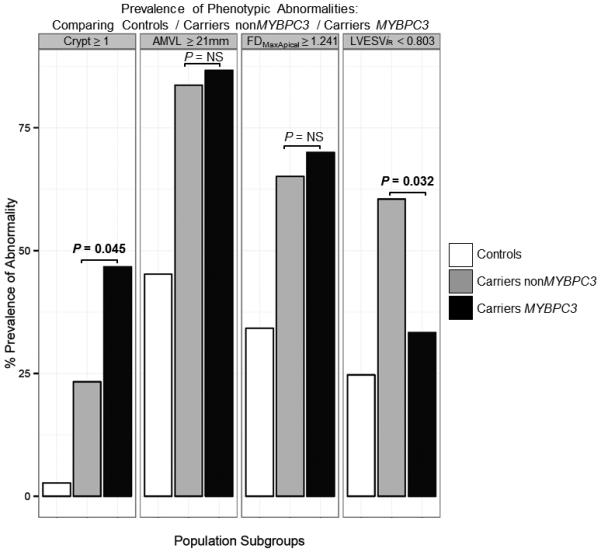
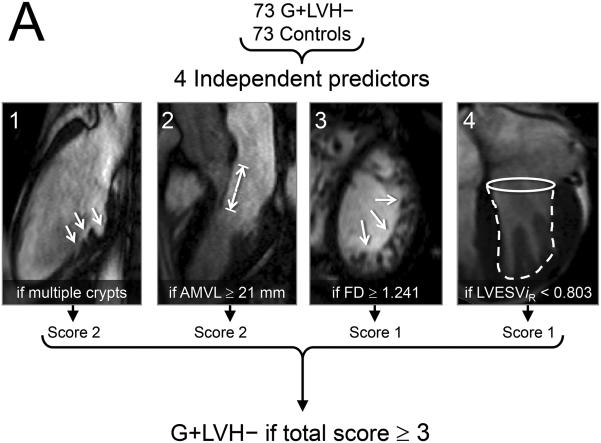
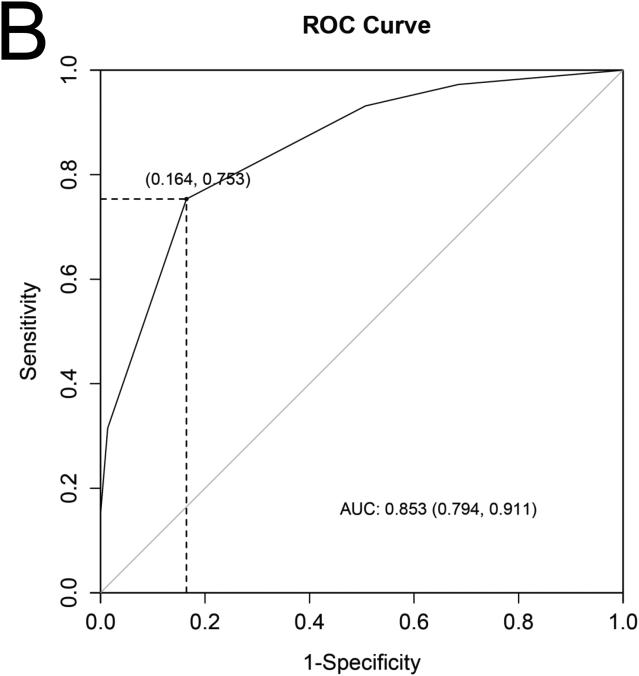
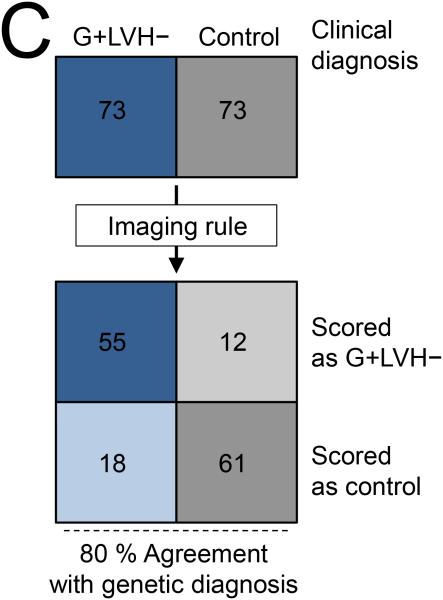
Methods and results: A multicenter case-control study investigated crypts and 22 other cardiovascular magnetic resonance parameters in subclinical hypertrophic cardiomyopathy to determine their strength of association with sarcomere gene mutation carriage. The G+LVH- sample (n=73) was 29 ± 13 years old and 51% were men. Crypts were related to the presence of sarcomere mutations (for ≥1 crypt, β=2.5; 95% confidence interval [CI], 0.5-4.4; P=0.014 and for ≥2 crypts, β=3.0; 95% CI, 0.8-7.9; P=0.004). In combination with 3 other parameters: anterior mitral valve leaflet elongation (β=2.1; 95% CI, 1.7-3.1; P<0.001), abnormal LV apical trabeculae (β=1.6; 95% CI, 0.8-2.5; P<0.001), and smaller LV end-systolic volumes (β=1.4; 95% CI, 0.5-2.3; P=0.001), multiple crypts indicated the presence of sarcomere gene mutations with 80% accuracy and an area under the curve of 0.85 (95% CI, 0.8-0.9). In this G+LVH- population, cardiac myosin-binding protein C mutation carriers had twice the prevalence of crypts when compared with the other combined mutations (47 versus 23%; odds ratio, 2.9; 95% CI, 1.1-7.9; P=0.045).
Conclusions: The subclinical hypertrophic cardiomyopathy phenotype measured by cardiovascular magnetic resonance in a multicenter environment and consisting of crypts (particularly multiple), anterior mitral valve leaflet elongation, abnormal trabeculae, and smaller LV systolic cavity is indicative of the presence of sarcomere gene mutations and highlights the need for further study.
Keywords: cardiomyopathy, hypertrophic; genetics; magnetic resonance imaging.
© 2014 American Heart Association, Inc.
Figures
References
-
- Maron BJ, Shirani J, Poliac LC, Mathenge R, Roberts WC, Mueller FO. Sudden death in young competitive athletes. Clinical, demographic, and pathological profiles. JAMA. 1996;276:199–204. - PubMed
-
- Maron BJ, Seidman JG, Seidman CE. Proposal for contemporary screening strategies in families with hypertrophic cardiomyopathy. J Am Coll Cardiol. 2004;44:2125–32. - PubMed
-
- Deva DP, Williams LK, Care M, Siminovitch KA, Moshonov H, Wintersperger BJ, Rakowski H, Crean AM. Deep basal inferoseptal crypts occur more commonly in patients with hypertrophic cardiomyopathy due to disease-causing myofilament mutations. Radiology. 2013;269:68–76. - PubMed
-
- Maron MS, Olivotto I, Harrigan C, Appelbaum E, Gibson CM, Lesser R, Haas TS, Udelson JE, Manning WJ, Maron BJ. Mitral valve abnormalities identified by cardiovascular magnetic resonance represent a primary phenotypic expression of hypertrophic cardiomyopathy. Circ. 2011;124:40–7. - PubMed
-
- Captur G, Lopes L, Patel V, Li C, Bassett P, Syrris P, Sado DM, Maestrini V, Mohun TJ, McKenna WJ, Muthurangu V, Elliott PM, Moon JC. Abnormal cardiac formation in hypertrophic cardiomyopathy - fractal analysis of trabeculae and preclinical gene expression. Circ Cardiovasc Genet. 2014;7:241–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
