

Molecular biology, pathogenesis and pathology of mumps virus
- PMID: 25229387
- PMCID: PMC4268314
- DOI: 10.1002/path.4445
Molecular biology, pathogenesis and pathology of mumps virus
Abstract
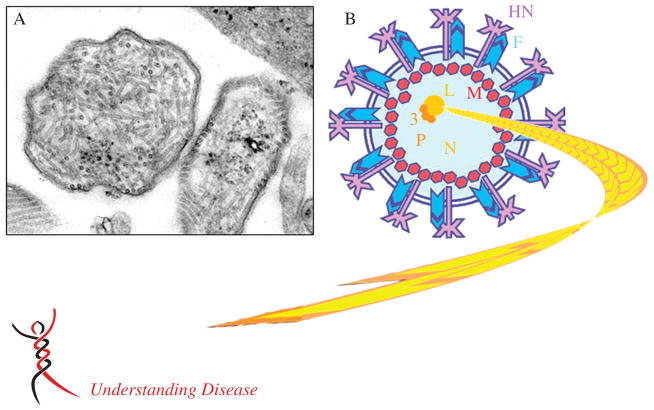
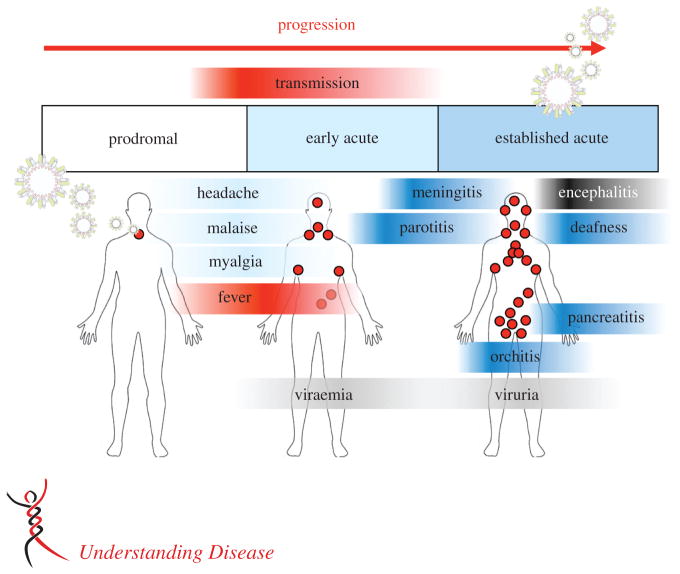
Mumps is caused by the mumps virus (MuV), a member of the Paramyxoviridae family of enveloped, non-segmented, negative-sense RNA viruses. Mumps is characterized by painful inflammatory symptoms, such as parotitis and orchitis. The virus is highly neurotropic, with laboratory evidence of central nervous system (CNS) infection in approximately half of cases. Symptomatic CNS infection occurs less frequently; nonetheless, prior to the introduction of routine vaccination, MuV was a leading cause of aseptic meningitis and viral encephalitis in many developed countries. Despite being one of the oldest recognized diseases, with a worldwide distribution, surprisingly little attention has been given to its study. Cases of aseptic meningitis associated with some vaccine strains and a global resurgence of cases, including in highly vaccinated populations, has renewed interest in the virus, particularly in its pathogenesis and the need for development of clinically relevant models of disease. In this review we summarize the current state of knowledge on the virus, its pathogenesis and its clinical and pathological outcomes.
Keywords: mumps; mumps virus; neurovirulence; pathogenesis; vaccine.
Copyright © 2014 Pathological Society of Great Britain and Ireland. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
No conflicts of interest were declared.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
