

Technical performance evaluation of the MyT4 point of care technology for CD4+ T cell enumeration
- PMID: 25229408
- PMCID: PMC4167862
- DOI: 10.1371/journal.pone.0107410
Technical performance evaluation of the MyT4 point of care technology for CD4+ T cell enumeration
Abstract
Objective: Though absolute CD4+ T cell enumeration is the primary gateway to antiretroviral therapy initiation for HIV-positive patients in all developing countries, patient access to this critical diagnostic test is relatively poor. We technically evaluated the performance of a newly developed point-of-care CD4+ T cell technology, the MyT4, compared with conventional CD4+ T cell testing technologies.
Design: Over 250 HIV-positive patients were consecutively enrolled and their blood tested on the MyT4, BD FACSCalibur, and BD FACSCount.
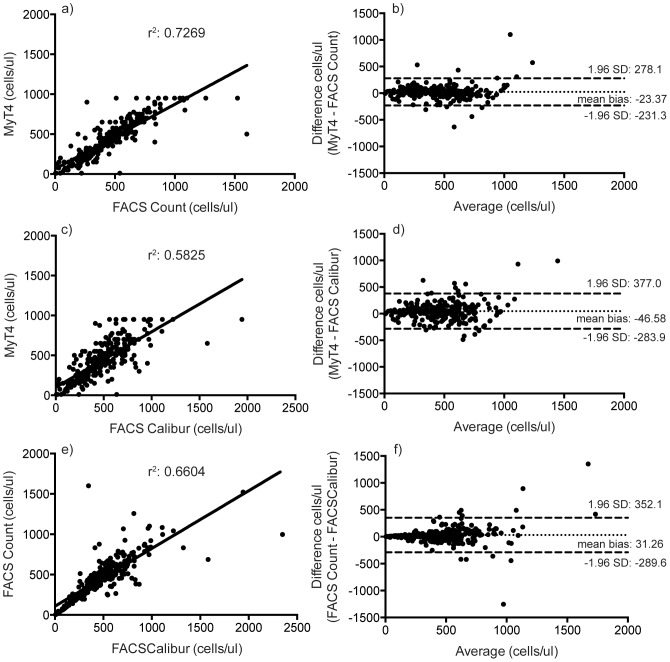
Results: Compared with the BD FACSCount, the MyT4 had an r2 of 0.7269 and a mean bias of -23.37 cells/µl. Compared with the BD FACSCalibur, the MyT4 had an r2 of 0.5825 and a mean bias of -46.58 cells/µl. Kenya currently uses a CD4+ T cell test threshold of 350 cells/µl to determine patient eligibility for antiretroviral therapy. At this threshold, the MyT4 had a sensitivity of 95.3% (95% CI: 88.4-98.7%) and a specificity of 87.9% (95% CI: 82.3-92.3%) compared with the BD FACSCount and sensitivity and specificity of 88.2% (95% CI: 79.4-94.2%) and 84.2% (95% CI: 78.2-89.2%), respectively, compared with the BD FACSCalibur. Finally, the MyT4 had a coefficient of variation of 12.80% compared with 14.03% for the BD FACSCalibur.
Conclusions: We conclude that the MyT4 performed well at the current 350 cells/µl ART initiation eligibility threshold when used by lower cadres of health care facility staff in rural clinics compared to conventional CD4+ T cell technologies.
Conflict of interest statement
Figures
References
-
- World Health Organization (2013) Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection: Recommendations for a Public Health Approach. - PubMed
-
- SMART Study Group, Emery S, Neuhaus JA, Phillips AN, Babiker A, et al. (2008) Major clinical outcomes in antiretroviral therapy (ART)-naive participants and in those not receiving ART at baseline in the SMART study. J Infect Dis 197: 1133–1144. - PubMed
-
- O'Brien WA, Hartigan PM, Martin D, Esinhart J, Hill A, et al. (1996) Changes in plasma HIV-1 RNA and CD4+ lymphocyte counts and the risk of progression to AIDS. Veterans Affairs Cooperative Study Group on AIDS. N Engl J Med 334: 426–431. - PubMed
-
- Post FA, Wood R, Maartens G (1996) CD4 and total lymphocyte counts as predictors of HIV disease progression. QJM 89: 505–508. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
