

Posttraumatic stress disorder symptoms and food addiction in women by timing and type of trauma exposure
- PMID: 25230359
- PMCID: PMC4341890
- DOI: 10.1001/jamapsychiatry.2014.1208
Posttraumatic stress disorder symptoms and food addiction in women by timing and type of trauma exposure
Abstract
Importance: Posttraumatic stress disorder (PTSD) appears to increase obesity risk but the pathways by which PTSD leads to weight gain are not known. Identification of the links between PTSD and obesogenic eating behaviors is necessary to clarify this pathway and inform development of obesity prevention strategies in PTSD-affected populations.
Objective: To determine whether women with PTSD symptoms are more likely to report food addiction, a measure of perceived dependence on food, than women without PTSD symptoms. Also, to determine whether age at PTSD symptom onset and type of trauma influence the PTSD-food addiction association.
Design, setting, and participants: Cross-sectional analysis of 49,408 participants in the Nurses' Health Study II, a cohort comprising women nurses who were aged 25 to 42 years at the 1989 recruitment from 14 US states.
Main outcomes and measures: The Nurses' Health Study II ascertained lifetime trauma exposure and PTSD symptoms in 2008 and current food addiction in 2009. Food addiction was defined as 3 or more clinically significant symptoms on a modified version of the Yale Food Addiction Scale. Confounder-adjusted prevalence ratios and 95% CIs were estimated using modified Poisson regression.
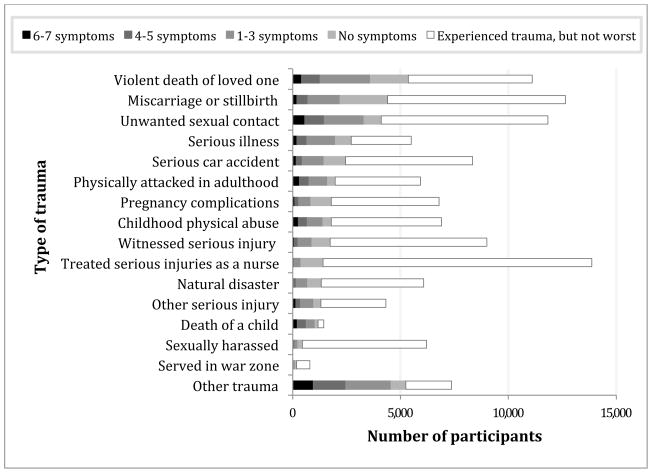
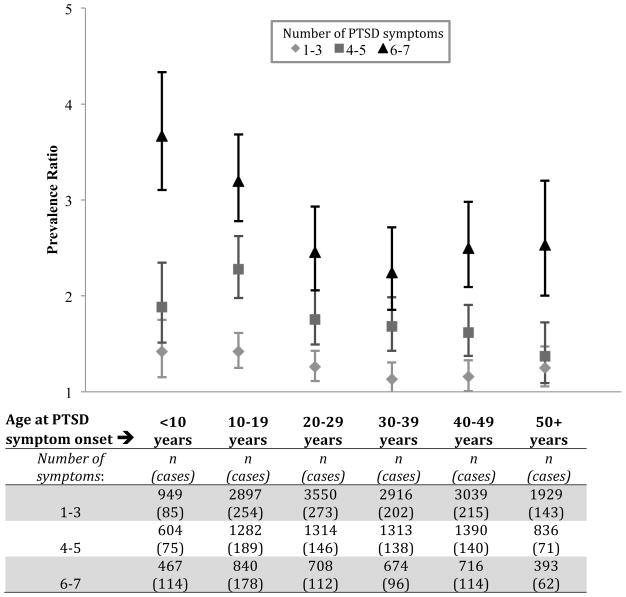
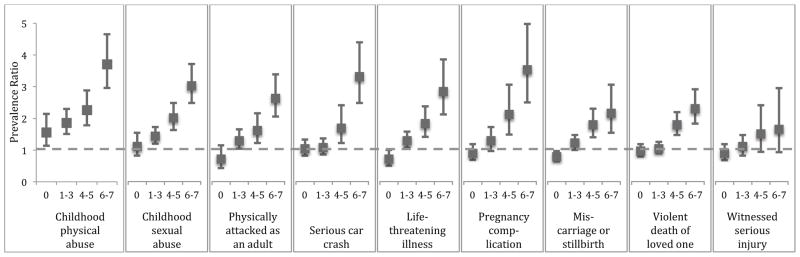
Results: Approximately 80% of the study sample reported some type of trauma exposure, with 66% of the trauma-exposed participants reporting at least 1 lifetime PTSD symptom. Eight percent of the cohort met the criteria for food addiction. The prevalence of food addiction increased with the number of lifetime PTSD symptoms, and women with the greatest number of PTSD symptoms (6-7 symptoms) had more than twice the prevalence of food addiction as women with neither PTSD symptoms nor trauma histories (prevalence ratio, 2.68; 95% CI, 2.41-2.97). Symptoms of PTSD were more strongly related to food addiction when symptom onset occurred at an earlier age. The PTSD-food addiction association did not differ substantially by trauma type.
Conclusions and relevance: Symptoms of PTSD were associated with increased food addiction prevalence in this cohort of women. Strategies to reduce obesity associated with PTSD may require psychological and behavioral interventions that address dependence on food and/or use of food to cope with distress.
Conflict of interest statement
Figures
References
-
- Thomas JL, Wilk JE, Riviere LA, McGurk D, Castro CA, Hoge CW. Prevalence of mental health problems and functional impairment among active component and National Guard soldiers 3 and 12 months following combat in Iraq. Arch Gen Psychiatry. 2010;67(6):614–23. - PubMed
-
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62:593–602. - PubMed
-
- Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry. 1995;52:1048–1060. - PubMed
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4. 2000. p. 943. Text Revision.
-
- Resnick HS, Kilpatrick DG, Dansky BS, Saunders BE, Best CL. Prevalence of civilian trauma and posttraumatic stress disorder in a representative national sample of women. J Consult Clin Psychol. 1993;61:984–991. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
