

Multicenter prospective clinical study to evaluate the prediction of short-term outcome in pregnant women with suspected preeclampsia (PROGNOSIS): study protocol
- PMID: 25230734
- PMCID: PMC4262142
- DOI: 10.1186/1471-2393-14-324
Multicenter prospective clinical study to evaluate the prediction of short-term outcome in pregnant women with suspected preeclampsia (PROGNOSIS): study protocol
Abstract
Background: Preeclampsia is defined as new onset of hypertension and proteinuria at gestational week 20 or after. However, use of these measures to predict preeclampsia before its clinical onset is unreliable, and evidence suggests that preeclampsia, eclampsia, or hemolysis, elevated liver enzymes and low platelet count (HELLP) syndrome may develop without hypertension or proteinuria being evident. Because of its unpredictability, varying clinical presentation and potential adverse outcomes, pregnant women with suspected preeclampsia require intensive monitoring or hospitalization. Beyond preeclampsia diagnosis, there is a high unmet medical need for more reliable predictive markers for preeclampsia to improve maternal and fetal outcomes and reduce unnecessary hospital admissions. An imbalance of circulating angiogenic and antiangiogenic factors, including raised soluble fms-like tyrosine kinase-1 (sFlt-1) and decreased placental growth factor (PlGF), has been found in women diagnosed with preeclampsia and before clinical onset of the disease. The PRediction of short-term Outcome in preGNant wOmen with Suspected preeclampsIa Study (PROGNOSIS) was designed to investigate the use of the sFlt-1/PlGF ratio in the short-term prediction of preeclampsia.
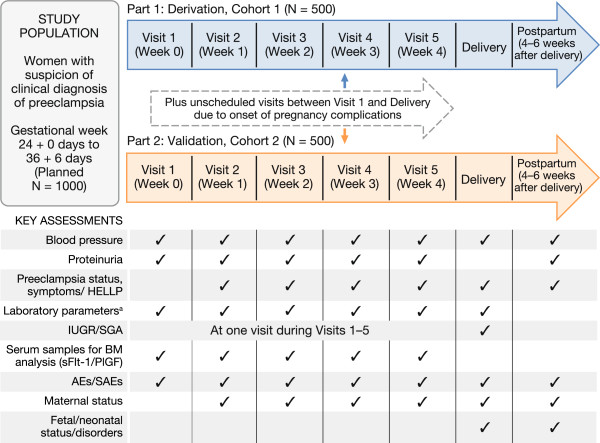
Methods/design: This global, multicenter, prospective, double-blind, non-interventional study aims to derive and validate cutoffs for the sFlt-1/PlGF ratio, to rule out (for 1 week) or rule in (within 4 weeks) the occurrence of preeclampsia/eclampsia/HELLP syndrome. Eligible participants are women presenting at 24 to <37 weeks' gestation with clinical suspicion of, but not manifest preeclampsia/eclampsia/HELLP syndrome. Clinical assessments, maternal serum sFlt-1/PlGF sampling and documentation of maternal/neonatal outcomes are performed at regular intervals, using strict diagnostic criteria for preeclampsia-related conditions and outcomes. Serum sFlt-1 and PlGF analysis will be performed using fully automated Elecsys® immunoassays. Investigators and participants will remain blinded to the results. Target recruitment is 1000 participants. Health economic analysis is also planned.
Discussion: The results of PROGNOSIS will provide the most comprehensive evidence to date on the accuracy of the sFlt-1/PlGF ratio for short-term prediction of preeclampsia/eclampsia/HELLP syndrome. Adoption of the sFlt-1/PlGF test in clinical practice has the potential to reduce the frequency of adverse pregnancy outcomes for both mother and fetus, and decrease healthcare costs associated with unnecessary hospitalization of women with suspected preeclampsia.
Figures
References
-
- Brown MA, Lindheimer MD, de Swiet M, Van Assche A, Moutquin JM. The classification and diagnosis of the hypertensive disorders of pregnancy: statement from the International Society for the Study of Hypertension in Pregnancy (ISSHP) Hypertens Pregnancy. 2001;20:IX–XIV. doi: 10.3109/10641950109152635. - DOI - PubMed
-
- Milne F, Redman C, Walker J, Baker P, Bradley J, Cooper C, de Swiet M, Fletcher G, Jokinen M, Murphy D, Nelson-Piercy C, Osgood V, Robson S, Shennan A, Tuffnell A, Twaddle S, Waugh J. The pre-eclampsia community guideline (PRECOG): how to screen for and detect onset of pre-eclampsia in the community. BMJ. 2005;330:576–580. doi: 10.1136/bmj.330.7491.576. - DOI - PMC - PubMed
-
- Lim K-H Medscape Reference Diseases and Conditions article.Preeclampsia Updated 18 November 2013. [ http://emedicine.medscape.com/article/1476919-overview#aw2aab6b3] (Accessed 11 December 2013)
-
- NICE clinical guideline 107 Last modified: January 2011.Hypertension in Pregnancy [ http://www.nice.org.uk/nicemedia/live/13098/50418/50418.pdf] (Accessed 25 November 2013).
Pre-publication history
-
- The pre-publication history for this paper can be accessed here: http://www.biomedcentral.com/1471-2393/14/324/prepub
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
