

Chronic traumatic encephalopathy: clinical-biomarker correlations and current concepts in pathogenesis
- PMID: 25231386
- PMCID: PMC4249716
- DOI: 10.1186/1750-1326-9-37
Chronic traumatic encephalopathy: clinical-biomarker correlations and current concepts in pathogenesis
Abstract
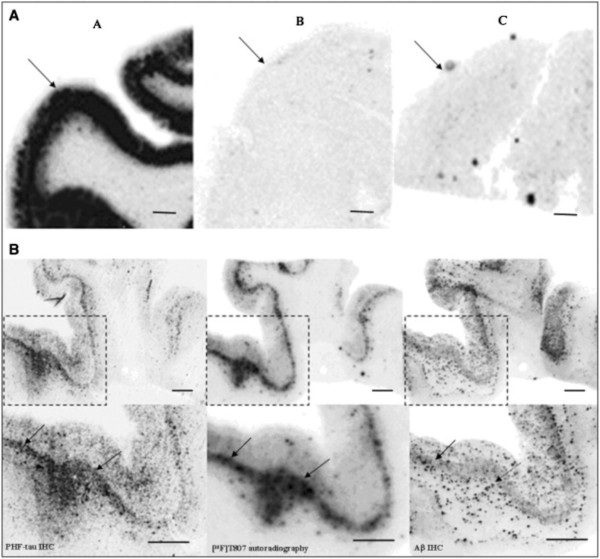
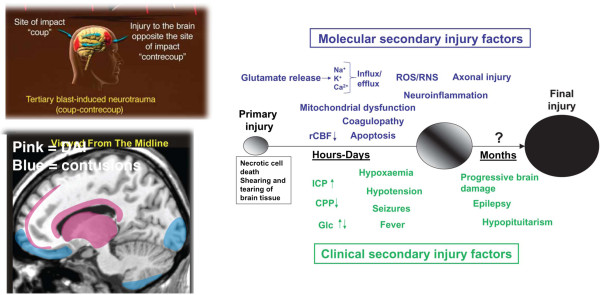
Background: Chronic traumatic encephalopathy (CTE) is a recently revived term used to describe a neurodegenerative process that occurs as a long term complication of repetitive mild traumatic brain injury (TBI). Corsellis provided one of the classic descriptions of CTE in boxers under the name "dementia pugilistica" (DP). Much recent attention has been drawn to the apparent association of CTE with contact sports (football, soccer, hockey) and with frequent battlefield exposure to blast waves generated by improvised explosive devices (IEDs). Recently, a promising serum biomarker has been identified by measurement of serum levels of the neuronal microtubule associated protein tau. New positron emission tomography (PET) ligands (e.g., [18 F] T807) that identify brain tauopathy have been successfully deployed for the in vitro and in vivo detection of presumptive tauopathy in the brains of subjects with clinically probable CTE.
Methods: Major academic and lay publications on DP/CTE were reviewed beginning with the 1928 paper describing the initial use of the term CTE by Martland.
Results: The major current concepts in the neurological, psychiatric, neuropsychological, neuroimaging, and body fluid biomarker science of DP/CTE have been summarized. Newer achievements, such as serum tau and [18 F] T807 tauopathy imaging, are also introduced and their significance has been explained.
Conclusion: Recent advances in the science of DP/CTE hold promise for elucidating a long sought accurate determination of the true prevalence of CTE. This information holds potentially important public health implications for estimating the risk of contact sports in inflicting permanent and/or progressive brain damage on children, adolescents, and adults.
Figures
Similar articles
-
Chronic traumatic encephalopathy: contributions from the Boston University Center for the Study of Traumatic Encephalopathy.Brain Inj. 2015;29(2):154-63. doi: 10.3109/02699052.2014.965215. Brain Inj. 2015. PMID: 25587744 Review.
-
Traumatic brain injury (TBI) in collision sports: Possible mechanisms of transformation into chronic traumatic encephalopathy (CTE).Metabolism. 2019 Nov;100S:153943. doi: 10.1016/j.metabol.2019.07.007. Metabolism. 2019. PMID: 31610856 Review.
-
[Late-onset Neurodegenerative Diseases Following Traumatic Brain Injury: Chronic Traumatic Encephalopathy (CTE) and Alzheimer's Disease Secondary to TBI (AD-TBI)].Brain Nerve. 2016 Jul;68(7):849-57. doi: 10.11477/mf.1416200517. Brain Nerve. 2016. PMID: 27395469 Japanese.
-
Tauopathy PET and amyloid PET in the diagnosis of chronic traumatic encephalopathies: studies of a retired NFL player and of a man with FTD and a severe head injury.Transl Psychiatry. 2014 Sep 16;4(9):e441. doi: 10.1038/tp.2014.91. Transl Psychiatry. 2014. PMID: 25226550 Free PMC article.
-
Cerebral [18 F]T807/AV1451 retention pattern in clinically probable CTE resembles pathognomonic distribution of CTE tauopathy.Transl Psychiatry. 2016 Sep 27;6(9):e900. doi: 10.1038/tp.2016.175. Transl Psychiatry. 2016. PMID: 27676441 Free PMC article.
Cited by
-
Neuroimaging assessment of early and late neurobiological sequelae of traumatic brain injury: implications for CTE.Front Neurosci. 2015 Sep 24;9:334. doi: 10.3389/fnins.2015.00334. eCollection 2015. Front Neurosci. 2015. PMID: 26441507 Free PMC article. Review.
-
Chronic Traumatic Encephalopathy: Update on Current Clinical Diagnosis and Management.Biomedicines. 2021 Apr 12;9(4):415. doi: 10.3390/biomedicines9040415. Biomedicines. 2021. PMID: 33921385 Free PMC article. Review.
-
Functional, Structural, and Neurotoxicity Biomarkers in Integrative Assessment of Concussions.Front Neurol. 2016 Oct 5;7:172. doi: 10.3389/fneur.2016.00172. eCollection 2016. Front Neurol. 2016. PMID: 27761129 Free PMC article.
-
Anatomical and Physiological Differences between Children and Adults Relevant to Traumatic Brain Injury and the Implications for Clinical Assessment and Care.Front Neurol. 2017 Dec 14;8:685. doi: 10.3389/fneur.2017.00685. eCollection 2017. Front Neurol. 2017. PMID: 29312119 Free PMC article. Review.
-
Cryptic Sites in Tau Fibrils Explain the Preferential Binding of the AV-1451 PET Tracer toward Alzheimer's Tauopathy.ACS Chem Neurosci. 2021 Jul 7;12(13):2437-2447. doi: 10.1021/acschemneuro.0c00340. Epub 2021 Jun 21. ACS Chem Neurosci. 2021. PMID: 34152739 Free PMC article.
References
-
- Martland HS. Punch drunk. JAMA. 1928;91:1103–1107.
-
- Millspaugh JA. Dementia pugilistica. US Naval Med Bull. 1937;35:297–303.
-
- Corsellis JAN, Bruton CJ, Freeman-Browne D. The aftermath of boxing. Psychol Med. 1973;3:270–303. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P01AG14449/AG/NIA NIH HHS/United States
- R01 AG043375/AG/NIA NIH HHS/United States
- P01 AG014449/AG/NIA NIH HHS/United States
- P50 AG005133/AG/NIA NIH HHS/United States
- I01 RX000684/RX/RRD VA/United States
- I01 CX000190/CX/CSRD VA/United States
- P01 AG025204/AG/NIA NIH HHS/United States
- P01AG25204/AG/NIA NIH HHS/United States
- I01 BX000348/BX/BLRD VA/United States
- P50AG05133/AG/NIA NIH HHS/United States
- I01 RX000179/RX/RRD VA/United States
- P01NS30318/NS/NINDS NIH HHS/United States
- I01 RX000511/RX/RRD VA/United States
- P01 NS030318/NS/NINDS NIH HHS/United States
- I01 RX000996/RX/RRD VA/United States
- P50 AG005138/AG/NIA NIH HHS/United States
- P50 AG05138/AG/NIA NIH HHS/United States
- UL1-RR‐029887/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
