

Prevalence of myocardial crypts in a large retrospective cohort study by cardiovascular magnetic resonance
- PMID: 25231729
- PMCID: PMC4164788
- DOI: 10.1186/s12968-014-0066-0
Prevalence of myocardial crypts in a large retrospective cohort study by cardiovascular magnetic resonance
Abstract
Background: Myocardial crypts are discrete clefts or fissures in otherwise compacted myocardium of the left ventricle (LV). Recent reports suggest a higher prevalence of crypts in patients with hypertrophic cardiomyopathy (HCM) and also within small samples of genotype positive but phenotype negative relatives. The presence of a crypt has been suggested to be a predictor of gene carrier status. However, the prevalence and clinical significance of crypts in the general population is unclear. We aimed to determine the prevalence of myocardial crypts in a large cohort of subjects using clinical cardiovascular magnetic resonance (CMR).
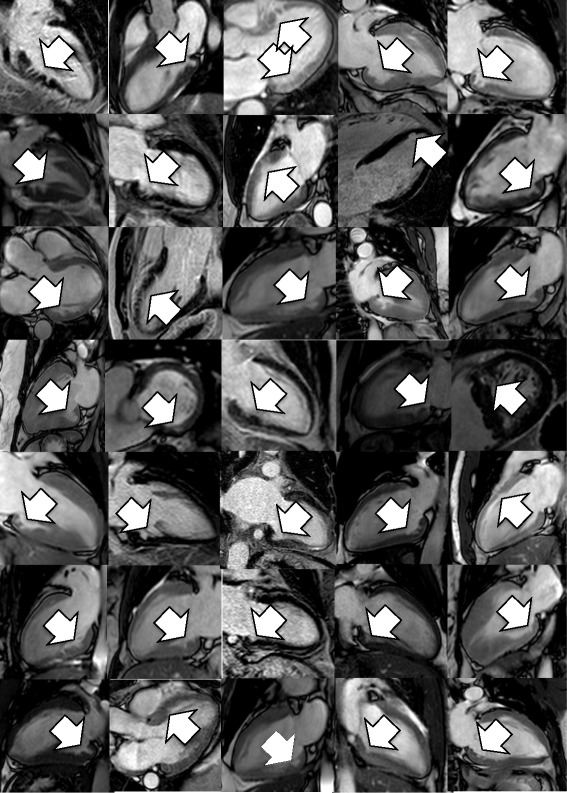
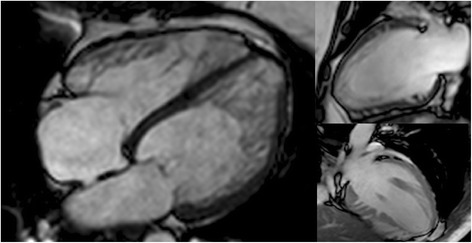
Methods: Consecutive subjects referred for clinical CMR during a 12-month period (n = 1020, age 52.6 ± 17, males: 61%) were included. Crypts were defined as >50% invagination into normal myocardium and their overall prevalence, location and shape was investigated and compared between different patient groups.
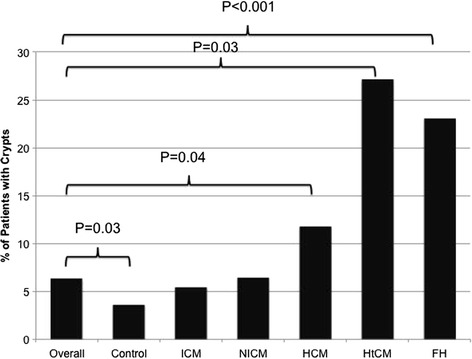
Results: The overall prevalence of crypts was 64/1020 (6.3%). In a predefined 'normal' control group the prevalence was lower (11/306, 3.6%, p = 0.031), but were equally prevalent in ischemic heart disease (12/236, 5.1%, p = n/s) and the combined non-ischemic cardiomyopathy (NICM) groups (24/373; 6.4%, p = n/s). Within the NICM group, crypts were significantly more common in HCM (9/76, 11.7%, p = 0.04) and hypertensive CM subjects (3/11, 27%, p = 0.03). In patients referred for CMR for family screening of inherited forms of CM, crypts were significantly more prevalent (10/41, 23%, p < 0.001), including a smaller group with a first degree relative with HCM (3/9, 33%, p = 0.01).
Conclusion: Myocardial crypts are relatively common in the normal population, and increasingly common in HCM and hypertensive cardiomyopathy. Crypts are also more frequently seen in normal phenotype subjects referred because of a family history of an inherited cardiomyopathy and HCM specifically. It is uncertain what the significance of crypts are in this group, and because of variability in the imaging protocols used and their relative frequency within the normal population, should not be used to clinically stratify these patients. Prospective studies are required to confirm the clinical significance of myocardial crypts, as their significance remains unclear.
Figures
References
-
- Bellenger NG, Burgess MI, Ray SG, Lahiri A, Coats AJ, Cleland JG, Pennell DJ. Comparison of left ventricular ejection fraction and volumes in heart failure by echocardiography, radionuclide ventriculography and cardiovascular magnetic resonance; are they interchangeable? Eur Heart J. 2000;21:1387–1396. doi: 10.1053/euhj.2000.2011. - DOI - PubMed
-
- Grothues F, Smith GC, Moon JC, Bellenger NG, Collins P, Klein HU, Pennell DJ. Comparison of interstudy reproducibility of cardiovascular magnetic resonance with two-dimensional echocardiography in normal subjects and in patients with heart failure or left ventricular hypertrophy. Am J Cardiol. 2002;90:29–34. doi: 10.1016/S0002-9149(02)02381-0. - DOI - PubMed
-
- Puntmann VO, Gebker R, Duckett S, Mirelis J, Schnackenburg B, Graefe M, Razavi R, Fleck E, Nagel E. Left ventricular chamber dimensions and wall thickness by cardiovascular magnetic resonance: comparison with transthoracic echocardiography. Euro Heart J Cardiovasc Imaging. 2013;14:240–246. doi: 10.1093/ehjci/jes145. - DOI - PubMed
-
- Puntmann VO, Jansen C, Nagel E. Letter by Puntmann et al. regarding article, "Prevalence and clinical profile of myocardial crypts in hypertrophic cardiomyopathy".Circ Cardiovasc Imaging. 2012; 5:author reply e7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
