

Experience with afatinib in patients with non-small cell lung cancer progressing after clinical benefit from gefitinib and erlotinib
- PMID: 25232040
- PMCID: PMC4200993
- DOI: 10.1634/theoncologist.2014-0103
Experience with afatinib in patients with non-small cell lung cancer progressing after clinical benefit from gefitinib and erlotinib
Abstract
Background: Afatinib, an irreversible ErbB family blocker, demonstrated superiority to chemotherapy as first-line treatment in patients with EGFR-mutated non-small cell lung cancer (NSCLC). Afatinib is also active in patients progressing on EGFR tyrosine kinase inhibitors (EGFR-TKIs). We report the results of a large cohort of NSCLC patients receiving afatinib within a compassionate-use program (CUP).
Patients and methods: Patients with advanced NSCLC progressing after one line or more of chemotherapy and one line or more of EGFR-TKI treatment with either an EGFR mutation or documented clinical benefit were enrolled. Data collection was not monitored or verified by central review. The intention of this CUP was to provide controlled preregistration access to afatinib for patients with life-threatening diseases and no other treatment option.
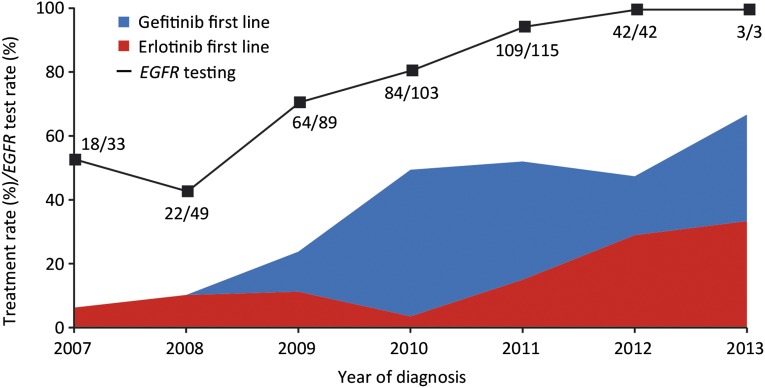
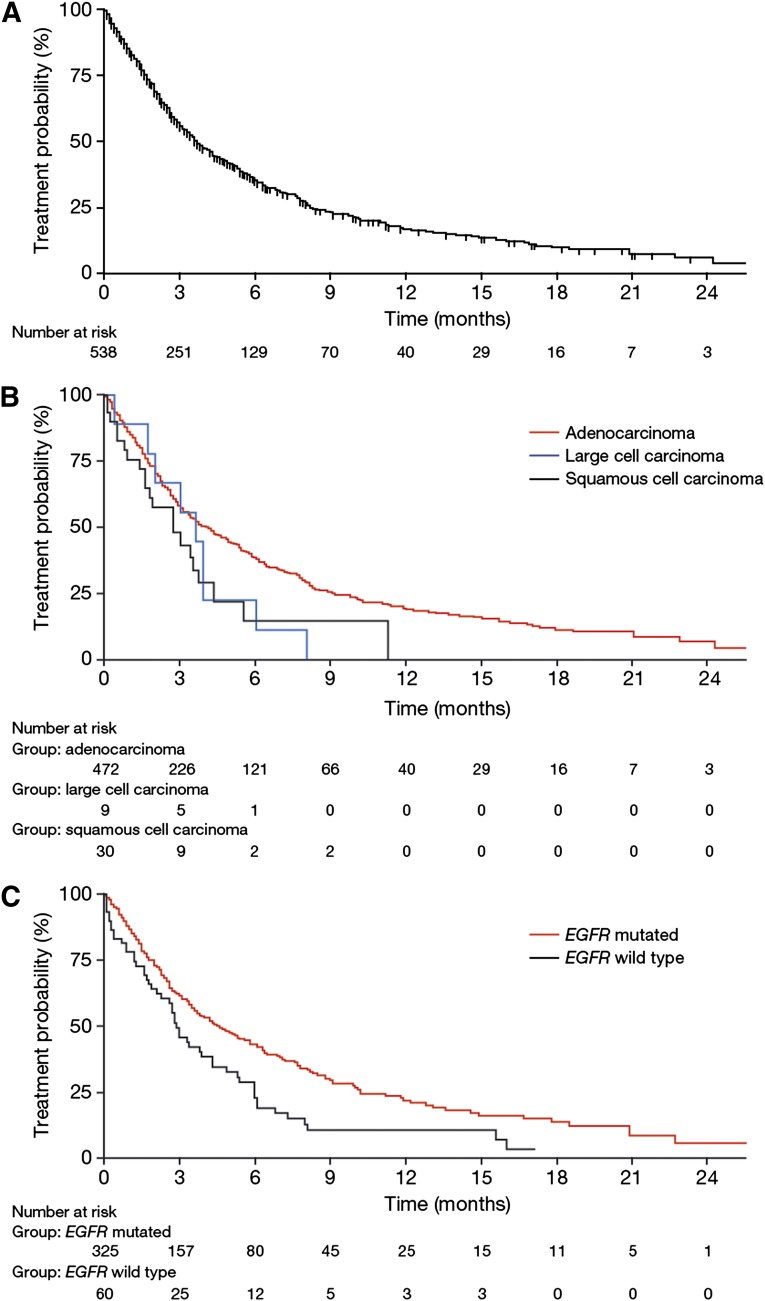
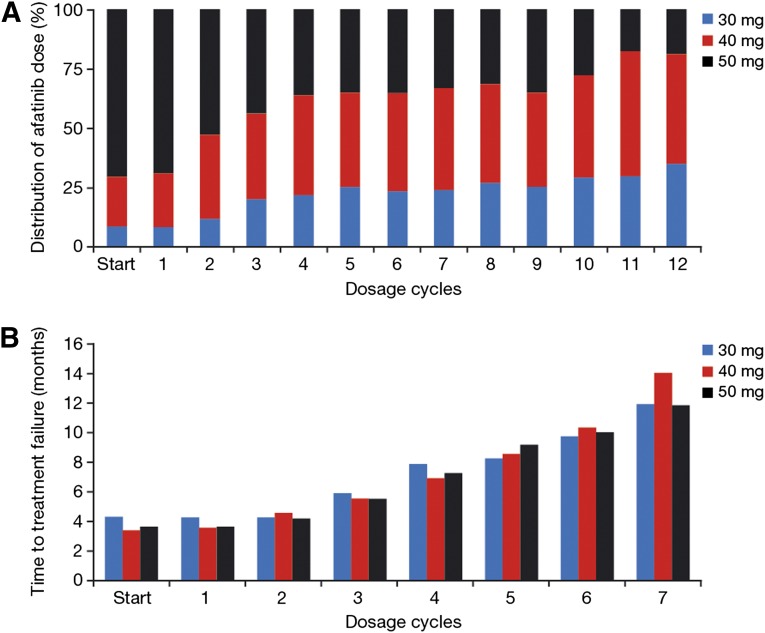
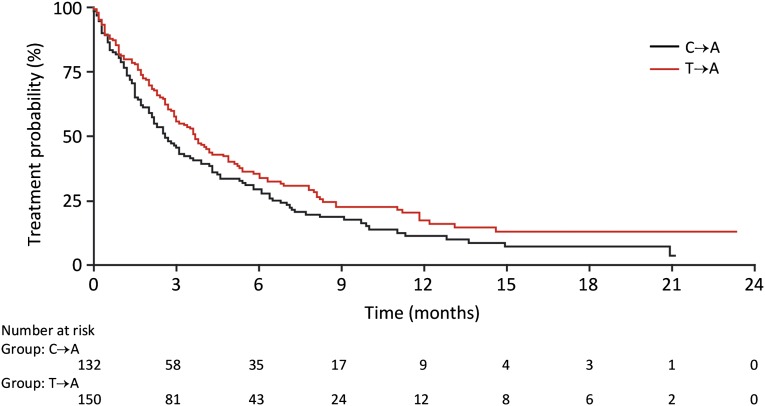
Results: From May 2010 to October 2013, 573 patients (65% female; median age: 64 years [range: 28-89 years]) were enrolled, with strong participation of community oncologists. Comorbidities were allowed, including second malignancies in 11% of patients. EGFR mutation status was available in 391 patients (72%), and 83% tested mutation positive. Median time to treatment failure (TTF) of 541 patients treated with afatinib was 3.7 months (range: 0.0 to >29.0 months). Median TTF was 4.0 and 2.7 months in patients with adenocarcinomas and squamous cell carcinomas, respectively, and 4.6 months in patients with EGFR-mutated NSCLC. Adverse events were generally manageable.
Conclusion: Afatinib was able to be given in a real-world setting to heavily pretreated patients with EGFR-mutated or EGFR-TKI-sensitive NSCLC. Acknowledging the constraints of data collection in a CUP, afatinib appears to be safe and to confer some clinical benefit in this population.
Keywords: Afatinib; Epidermal growth factor receptor; Erlotinib; Gefitinib; Non-small cell lung cancer.
©AlphaMed Press.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
References
-
- World cancer factsheet. Available at http://publications.cancerresearchuk.org/downloads/product/CS_FS_WORLD_A... Accessed February 28, 2014.
-
- Lynch TJ, Bell DW, Sordella R, et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med. 2004;350:2129–2139. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
