

doi: 10.1128/JCM.02306-14.
Epub 2014 Sep 17.
Evaluation of the BD Max MRSA XT assay for use with different swab types
Affiliations
- PMID: 25232162
- PMCID: PMC4313310
- DOI: 10.1128/JCM.02306-14
Item in Clipboard
Evaluation of the BD Max MRSA XT assay for use with different swab types
J Clin Microbiol.
2014 Dec.
Abstract
We evaluated the performance of the BD Max MRSA XT assay for use with different swab types. The 90% detection rates (95% confidence intervals) were 387 (97 to 1,551), 877 (238 to 3,230), 986 (183 to 5,287), 1,292 (328 to 5,078), 2,400 (426 to 13,518), and 5,848 (622 to 55,021) CFU/swab for Liquid Stuart, Liquid Amies, dry, Amies Gel without charcoal, ESwab collection, and Amies gel with charcoal swabs (Becton Dickinson), respectively. Amies Gel without charcoal, ESwab collection, and Amies gel with charcoal swabs had a tendency to be less sensitive, but none of the differences was statistically significant.
Copyright © 2014, American Society for Microbiology. All Rights Reserved.
Figures
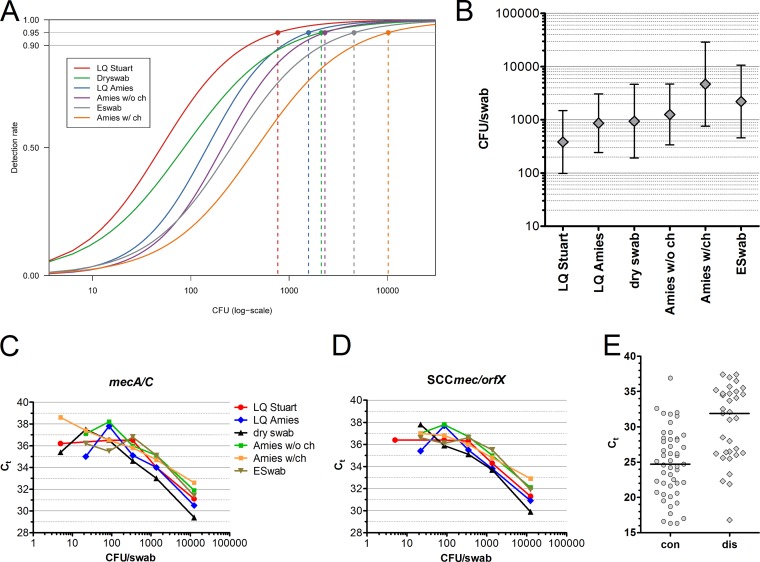
(A) Two-parameter log-logistic model-based curves for the frequency of positive MRSA results in dependency of the bacterial input per swab calculated for six different swab types. Shown are the limits of detection for 95% detection rate. The 90% detection level is also indicated. (B) Estimates for the LoD for the 90% detection rate and 95% confidence intervals for the various swabs. (C and D) Real-time PCR CT values for serial dilutions of MRSA and detection of mecA or mecC and SCCmec-orfX using the indicated swab types. (E) Distribution of CT values for SCCmec-orfX obtained with the BD Max MRSA assay in a clinical routine setting for samples that were confirmed by culture (concordant [con]) or were culture negative (discordant [dis]). Random selection of 49 concordant and 33 discordant results. Medians are shown. LQ, liquid; w/o ch, without charcoal; w/ch, with charcoal.
Similar articles
-
Comparison of ESwab and Wound Fiber Swab Specimen Collection Devices for Use with Xpert SA Nasal Complete Assay.J Clin Microbiol. 2016 Jul;54(7):1904-1906. doi: 10.1128/JCM.00449-16. Epub 2016 Apr 27. J Clin Microbiol. 2016. PMID: 27122376 Free PMC article.
-
Clinical evaluation of the Copan ESwab for methicillin-resistant Staphylococcus aureus detection and culture of wounds.Eur J Clin Microbiol Infect Dis. 2011 Aug;30(8):943-9. doi: 10.1007/s10096-011-1178-1. Epub 2011 Feb 6. Eur J Clin Microbiol Infect Dis. 2011. PMID: 21298460
-
Rapid detection of methicillin-resistant Staphylococcus aureus (MRSA) in diverse clinical specimens by the BD GeneOhm MRSA assay and comparison with culture.J Clin Microbiol. 2010 Mar;48(3):981-4. doi: 10.1128/JCM.01990-09. Epub 2010 Jan 13. J Clin Microbiol. 2010. PMID: 20071545 Free PMC article.
-
Automation of the BD GeneOhm methicillin-resistant Staphylococcus aureus assay for high-throughput screening of nasal swab specimens.J Clin Microbiol. 2009 May;47(5):1546-8. doi: 10.1128/JCM.00114-09. Epub 2009 Mar 18. J Clin Microbiol. 2009. PMID: 19297592 Free PMC article.
-
A common variant of staphylococcal cassette chromosome mec type IVa in isolates from Copenhagen, Denmark, is not detected by the BD GeneOhm methicillin-resistant Staphylococcus aureus assay.J Clin Microbiol. 2009 May;47(5):1524-7. doi: 10.1128/JCM.02153-08. Epub 2009 Mar 18. J Clin Microbiol. 2009. PMID: 19297600 Free PMC article.
Cited by
-
Evaluation of BD Max StaphSR and BD Max MRSAXT Assays Using ESwab-Collected Specimens.J Clin Microbiol. 2015 Aug;53(8):2525-9. doi: 10.1128/JCM.00970-15. Epub 2015 May 27. J Clin Microbiol. 2015. PMID: 26019193 Free PMC article.
-
Comparative Evaluation of Two PCR-Based Methods for Detection of Methicillin-Resistant Staphylococcus aureus (MRSA): Xpert MRSA Gen 3 and BD-Max MRSA XT.J Clin Microbiol. 2015 Jun;53(6):1955-8. doi: 10.1128/JCM.03679-14. Epub 2015 Apr 15. J Clin Microbiol. 2015. PMID: 25878336 Free PMC article.
-
Culture harder: use more specimens to increase methicillin-resistant Staphylococcus aureus culture yield relative to PCR.Access Microbiol. 2025 Jun 3;7(6):000918.v4. doi: 10.1099/acmi.0.000918.v4. eCollection 2025. Access Microbiol. 2025. PMID: 40475911 Free PMC article.
-
Evaluation of the BD Max StaphSR Assay for Rapid Identification of Staphylococcus aureus and Methicillin-Resistant S. aureus in Positive Blood Culture Broths.J Clin Microbiol. 2015 Nov;53(11):3630-2. doi: 10.1128/JCM.01922-15. Epub 2015 Aug 19. J Clin Microbiol. 2015. PMID: 26292311 Free PMC article.
-
Liquid and Dry Swabs for Culture- and PCR-Based Detection of Colonization with Methicillin-Resistant Staphylococcus aureus during Admission Screening.Eur J Microbiol Immunol (Bp). 2019 Dec 25;9(4):131-137. doi: 10.1556/1886.2019.00022. eCollection 2019 Dec 25. Eur J Microbiol Immunol (Bp). 2019. PMID: 31934365 Free PMC article.
References
-
- Brukner I, Oughton M, Giannakakis A, Kerzner R, Dascal A. 2013. Significantly improved performance of a multitarget assay over a commercial SCCmec-based assay for methicillin-resistant Staphylococcus aureus screening: applicability for clinical laboratories. J. Mol. Diagn. 15:577–580. 10.1016/j.jmoldx.2013.04.009. - DOI - PubMed
-
- Blanc DS, Basset P, Nahimana-Tessemo I, Jaton K, Greub G, Zanetti G. 2011. High proportion of wrongly identified methicillin-resistant Staphylococcus aureus carriers by use of a rapid commercial PCR assay due to presence of staphylococcal cassette chromosome element lacking the mecA gene. J. Clin. Microbiol. 49:722–724. 10.1128/JCM.01988-10. - DOI - PMC - PubMed
-
- Dalpke AH, Hofko M, Zimmermann S. 2012. Comparison of the BD Max methicillin-resistant Staphylococcus aureus (MRSA) assay and the BD GeneOhm MRSA achromopeptidase assay with direct- and enriched-culture techniques using clinical specimens for detection of MRSA. J. Clin. Microbiol. 50:3365–3367. 10.1128/JCM.01496-12. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
