

Radiology of pancreatic neoplasms: An update
- PMID: 25232458
- PMCID: PMC4163731
- DOI: 10.4251/wjgo.v6.i9.330
Radiology of pancreatic neoplasms: An update
Abstract
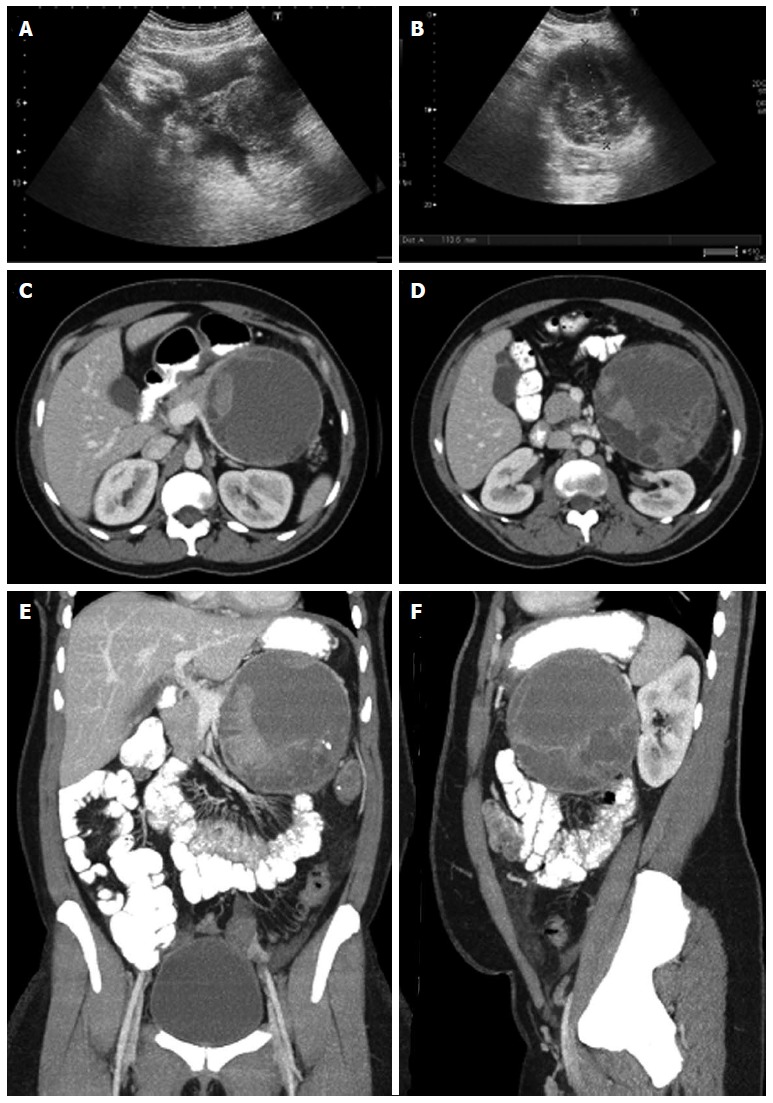
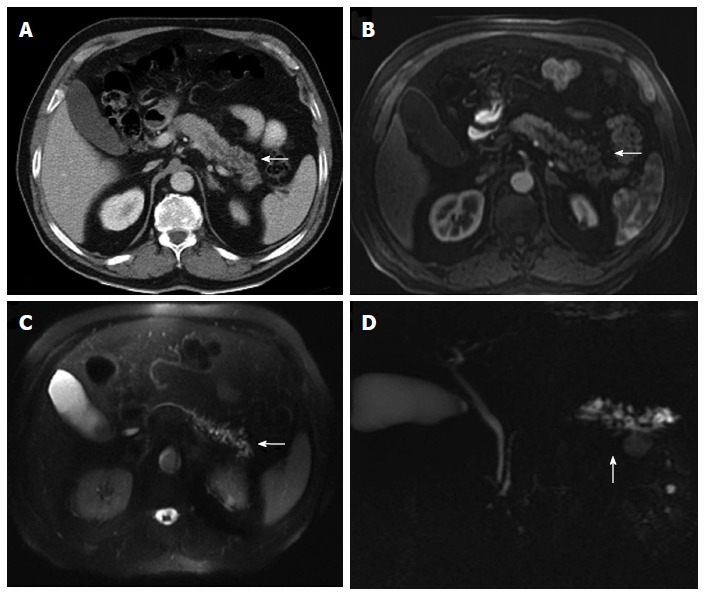
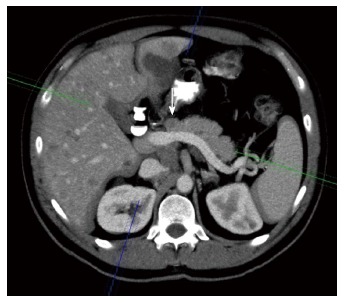
Diagnostic imaging is an important tool to evaluate pancreatic neoplasms. We describe the imaging features of pancreatic malignancies and their benign mimics. Accurate detection and staging are essential for ensuring appropriate selection of patients who will benefit from surgery and for preventing unnecessary surgeries in patients with unresectable disease. Ultrasound, multidetector computed tomography with multiplanar reconstruction and magnetic resonance imaging can help to do a correct diagnosis. Radiologists should be aware of the wide variety of anatomic variants and pathologic conditions that may mimic pancreatic neoplasms. The knowledge of the most important characteristic key findings may facilitate the right diagnosis.
Keywords: Computed tomography; Magnetic resonance imaging; Pancreas; Pancreatic neoplasms; Radiology; Surgery; cancer.
Figures


References
-
- Lu DS, Reber HA, Krasny RM, Kadell BM, Sayre J. Local staging of pancreatic cancer: criteria for unresectability of major vessels as revealed by pancreatic-phase, thin-section helical CT. AJR Am J Roentgenol. 1997;168:1439–1443. - PubMed
-
- Brennan DD, Zamboni GA, Raptopoulos VD, Kruskal JB. Comprehensive preoperative assessment of pancreatic adenocarcinoma with 64-section volumetric CT. Radiographics. 2007;27:1653–1666. - PubMed
-
- Low G, Panu A, Millo N, Leen E. Multimodality imaging of neoplastic and nonneoplastic solid lesions of the pancreas. Radiographics. 2011;31:993–1015. - PubMed
-
- Ros PR, Mortelé KJ. Imaging features of pancreatic neoplasms. JBR-BTR. 2001;84:239–249. - PubMed
-
- Ross BA, Jeffrey RB, Mindelzun RE. Normal variations in the lateral contour of the head and neck of the pancreas mimicking neoplasm: evaluation with dual-phase helical CT. AJR Am J Roentgenol. 1996;166:799–801. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
