

Complications of hip fractures: A review
- PMID: 25232517
- PMCID: PMC4133447
- DOI: 10.5312/wjo.v5.i4.402
Complications of hip fractures: A review
Abstract
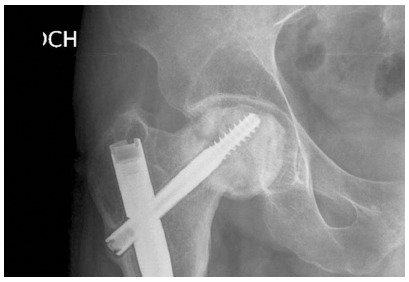
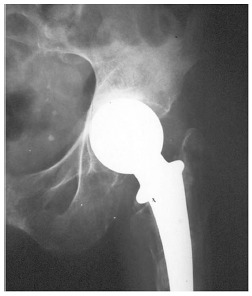
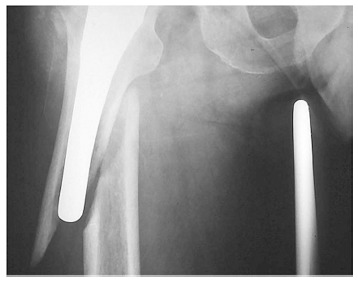
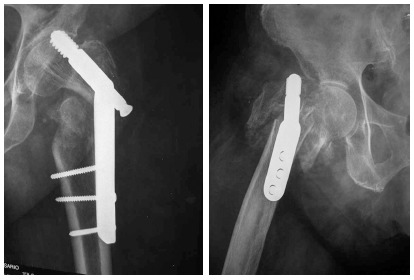
Nowadays, fracture surgery represents a big part of the orthopedic surgeon workload, and usually has associated major clinical and social cost implications. These fractures have several complications. Some of these are medical, and other related to the surgical treatment itself. Medical complications may affect around 20% of patients with hip fracture. Cognitive and neurological alterations, cardiopulmonary affections (alone or combined), venous thromboembolism, gastrointestinal tract bleeding, urinary tract complications, perioperative anemia, electrolytic and metabolic disorders, and pressure scars are the most important medical complications after hip surgery in terms of frequency, increase of length of stay and perioperative mortality. Complications arising from hip fracture surgery are fairly common, and vary depending on whether the fracture is intracapsular or extracapsular. The main problems in intracapsular fractures are biological: vascularization of the femoral head, and lack of periosteum -a major contributor to fracture healing- in the femoral neck. In extracapsular fractures, by contrast, the problem is mechanical, and relates to load-bearing. Early surgical fixation, the role of anti-thromboembolic and anti-infective prophylaxis, good pain control at the perioperative, detection and management of delirium, correct urinary tract management, avoidance of malnutrition, vitamin D supplementation, osteoporosis treatment and advancement of early mobilization to improve functional recovery and falls prevention are basic recommendations for an optimal maintenance of hip fractured patients.
Keywords: Anesthesia; Complications; Hip fracture; Morbidity; Mortality.
Figures





References
-
- British Orthopaedic Association. The care of patients with fragility fracture. London: British Orthopaedic Association; 2007. pp. 8–11.
-
- Auron-Gomez M, Michota F. Medical management of hip fracture. Clin Geriatr Med. 2008;24:701–719, ix. - PubMed
-
- Marsland D, Colvin PL, Mears SC, Kates SL. How to optimize patients for geriatric fracture surgery. Osteoporos Int. 2010;21:S535–S546. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
