

Impact of pretreatment imaging on survival of esophagectomy after induction therapy for esophageal cancer: who should be given the benefit of the doubt?: esophagectomy outcomes of patients with suspicious metastatic lesions
- PMID: 25234017
- PMCID: PMC4318780
- DOI: 10.1245/s10434-014-4079-6
Impact of pretreatment imaging on survival of esophagectomy after induction therapy for esophageal cancer: who should be given the benefit of the doubt?: esophagectomy outcomes of patients with suspicious metastatic lesions
Abstract
Purpose: We examined survival of patients who underwent esophagectomy for locally advanced esophageal cancer with foci that were suspicious for metastatic disease on initial imaging but whose disease did not progress after induction chemoradiation treatment (CRT).
Methods: The impact of pre- and posttherapy staging characteristics on survival of patients who underwent esophagectomy after CRT between 2003 and 2009 was evaluated using multivariable logistic regression. Survival of patients with and without possible metastatic disease on initial imaging was compared with the log-rank test.
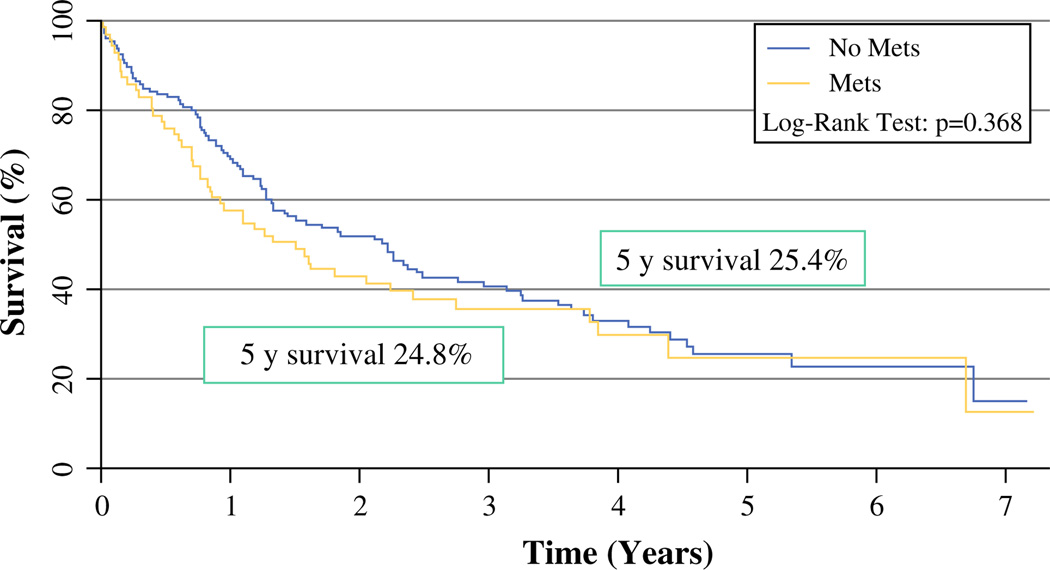
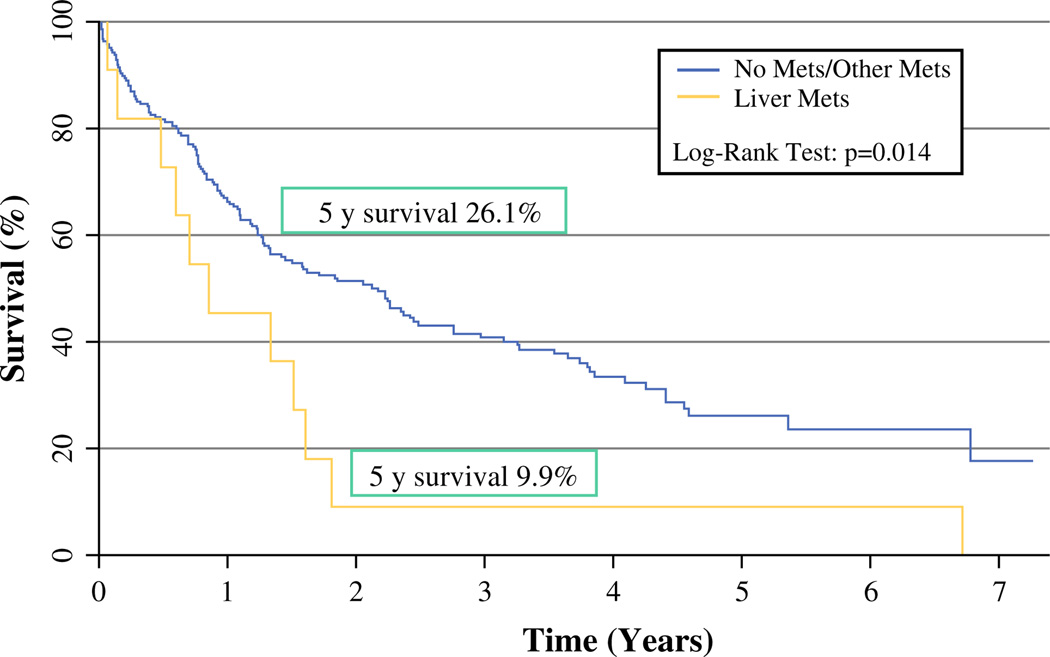
Results: During the study period, 71 (32%) of 220 patients who underwent CRT followed by esophagectomy had possible distant metastatic disease on initial imaging. Patients with initial suspicion of metastases had a 5-year survival of 24.8%. Overall survival of patients with and without possible metastatic disease on initial imaging was not significantly different (p = 0.4), but pretreatment positron emission tomography (PET) suggesting a liver lesion (hazard ratio [HR] 3.2, p = 0.003) predicted worse survival. Additional predictors of worse survival were clinical T4 status (HR 3.1, p = 0.001), post-CRT pathologic nodal status (HR 1.6, p = 0.04), and pathologically confirmed metastatic disease at or before resection (HR 3.1, p = 0.01). None of 10 patients with pathologic metastatic disease at resection lived longer than 2.5 years.
Conclusions: Patients with possible liver metastases on pretreatment PET and patients with confirmed metastatic disease at the time of surgery do not benefit from resection. However, patients with pretreatment imaging that shows possible metastatic disease in sites other than the liver still have reasonable long-term survival after resection.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Seigel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63:11–30. - PubMed
-
- Dubecz A, Gall I, Solymosi N, et al. Temporal trends in longterm survival and cure rates in esophageal cancer: a SEER database analysis. J Thorac Oncol. 2012;7:443–447. - PubMed
-
- Horner M, Ries L, Krapcho M, et al. SEER cancer statistics review, 1975–2006. Bethesda: National Cancer Institute; 2009. http://seer.cancer.gov/csr/1975_2006/, based on November 2008 SEER data submission, posted to the SEER Web site; 2009.
-
- Howlader N, Noone AM, Krapcho M, et al. SEER cancer statistics review, 1975–2008. Bethesda: National Cancer Institute; 2011. http://seer.cancer.gov/csr/1975_2008/, based on November 2010 SEER data submission, posted to the SEER Web site, 2011;
-
- Enzinger PC, Mayer RJ. Esophageal cancer. N Engl J Med. 2003;349:2241–2252. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
