

Offering lung cancer screening to high-risk medicare beneficiaries saves lives and is cost-effective: an actuarial analysis
- PMID: 25237423
- PMCID: PMC4163779
Offering lung cancer screening to high-risk medicare beneficiaries saves lives and is cost-effective: an actuarial analysis
Abstract
Background: By a wide margin, lung cancer is the most significant cause of cancer death in the United States and worldwide. The incidence of lung cancer increases with age, and Medicare beneficiaries are often at increased risk. Because of its demonstrated effectiveness in reducing mortality, lung cancer screening with low-dose computed tomography (LDCT) imaging will be covered without cost-sharing starting January 1, 2015, by nongrandfathered commercial plans. Medicare is considering coverage for lung cancer screening.
Objective: To estimate the cost and cost-effectiveness (ie, cost per life-year saved) of LDCT lung cancer screening of the Medicare population at high risk for lung cancer.
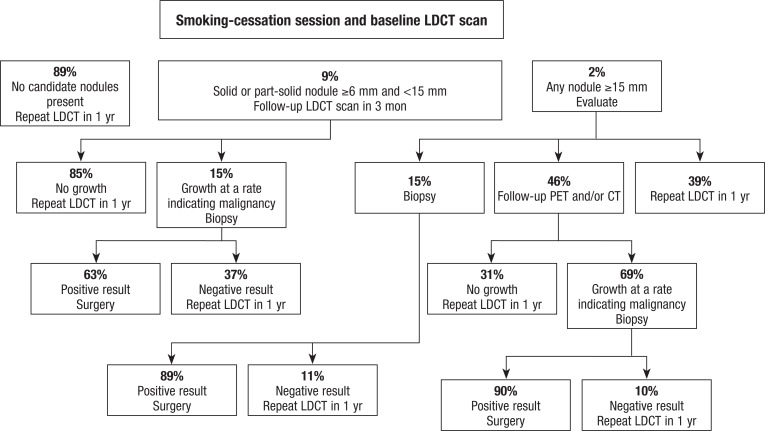
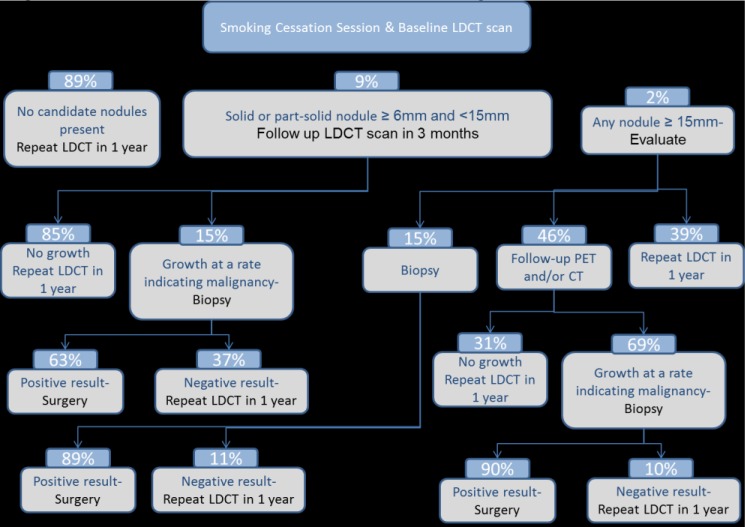
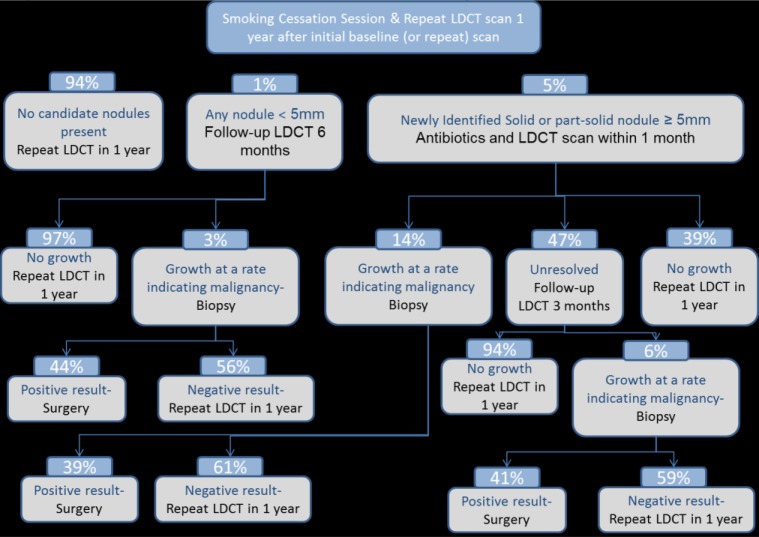
Methods: Medicare costs, enrollment, and demographics were used for this study; they were derived from the 2012 Centers for Medicare & Medicaid Services (CMS) beneficiary files and were forecast to 2014 based on CMS and US Census Bureau projections. Standard life and health actuarial techniques were used to calculate the cost and cost-effectiveness of lung cancer screening. The cost, incidence rates, mortality rates, and other parameters chosen by the authors were taken from actual Medicare data, and the modeled screenings are consistent with Medicare processes and procedures.
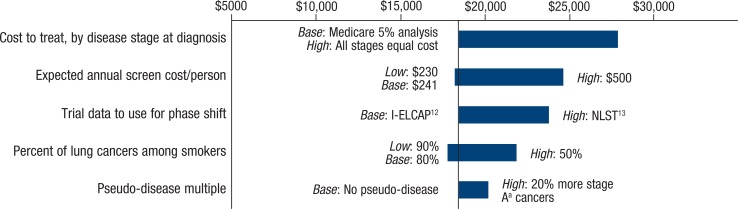
Results: Approximately 4.9 million high-risk Medicare beneficiaries would meet criteria for lung cancer screening in 2014. Without screening, Medicare patients newly diagnosed with lung cancer have an average life expectancy of approximately 3 years. Based on our analysis, the average annual cost of LDCT lung cancer screening in Medicare is estimated to be $241 per person screened. LDCT screening for lung cancer in Medicare beneficiaries aged 55 to 80 years with a history of ≥30 pack-years of smoking and who had smoked within 15 years is low cost, at approximately $1 per member per month. This assumes that 50% of these patients were screened. Such screening is also highly cost-effective, at <$19,000 per life-year saved.
Conclusion: If all eligible Medicare beneficiaries had been screened and treated consistently from age 55 years, approximately 358,134 additional individuals with current or past lung cancer would be alive in 2014. LDCT screening is a low-cost and cost-effective strategy that fits well within the standard Medicare benefit, including its claims payment and quality monitoring.
Figures
References
-
- American Cancer Society. Lung cancer (non-small cell) overview. Revised April 30, 2014. www.cancer.org/Cancer/LungCancer-Non-SmallCell/OverviewGuide/lung-cancer... Accessed June 6, 2014.
-
- American Lung Association. Lung cancer fact sheet. www.lung.org/lung-disease/lung-cancer/resources/facts-figures/lung-cance... Accessed July 21, 2014.
-
- American Cancer Society. What are the key statistics about lung cancer? Revised February 11, 2014. www.cancer.org/cancer/lungcancer-smallcell/detailedguide/small-cell-lung... Accessed June 17, 2014.
-
- Centers for Disease Control and Prevention. Lung cancer risk by age. Updated July 22, 2013. www.cdc.gov/cancer/lung/statistics/age.htm Accessed July 30, 2014.
-
- Ma J, Ward EM, Smith R, Jemal A. Annual number of lung cancer deaths potentially avertable by screening in the United States. Cancer. 2013; 119: 1381–1385 - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous