

Stereotactic aspiration versus craniotomy for primary intracerebral hemorrhage: a meta-analysis of randomized controlled trials
- PMID: 25237813
- PMCID: PMC4169548
- DOI: 10.1371/journal.pone.0107614
Stereotactic aspiration versus craniotomy for primary intracerebral hemorrhage: a meta-analysis of randomized controlled trials
Abstract
Background: A wealth of evidence based on the randomized controlled trials (RCTs) has indicated that surgery may be a better choice in the management of primary intracerebral hemorrhage (ICH) compared to conservative treatment. However, there is considerable controversy over selecting appropriate surgical procedures for ICH. Thus, this meta-analysis was performed to assess the effects of stereotactic aspiration compared to craniotomy in patients with ICH.
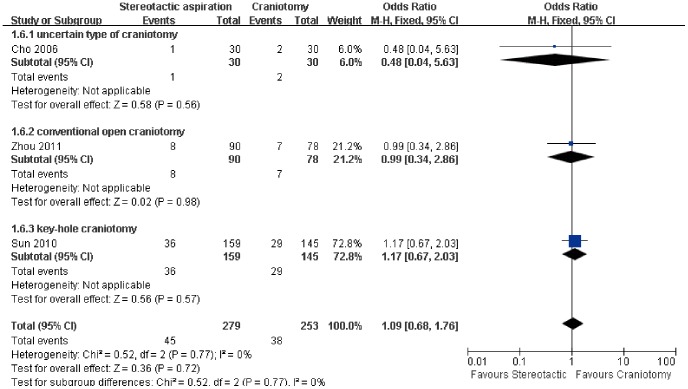
Methods: According to the study strategy, we searched PUBMED, EMBASE and Cochrane Central Register of Controlled Trials. Other sources such as the internet-based clinical trial registries, relevant journals and the lists of references were also searched. After literature searching, two investigators independently performed literature screening, assessment of quality of the included trials and data extraction. The outcome measures included death or dependence, total risk of complication, and the risk of rebleeding, gastrointestinal hemorrhage and systematic infection.
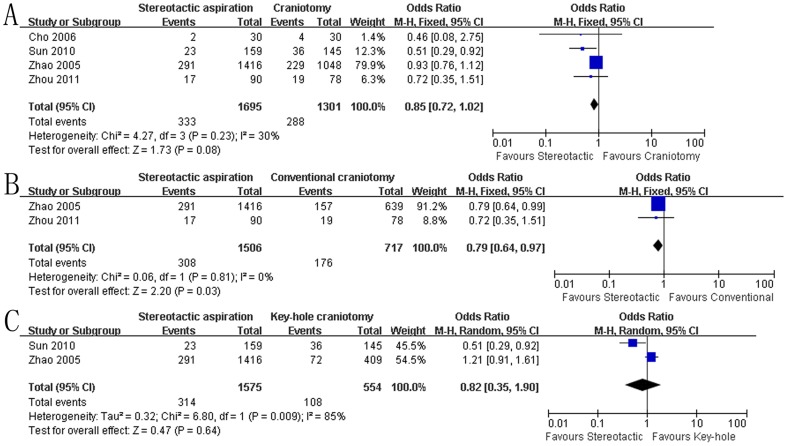
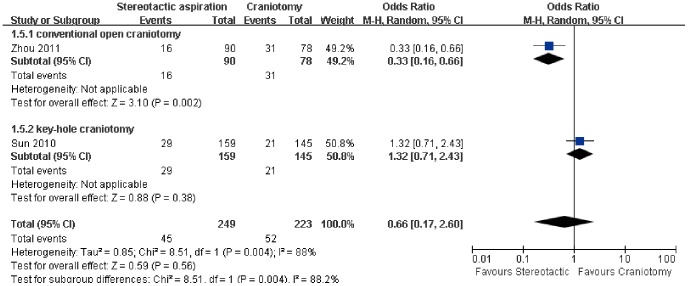
Results: Four RCTs with 2996 participants were included. The quality of the included trials was acceptable. Stereotactic aspiration significantly decreased the odds of death or dependence at the final follow-up (odds ratio (OR): 0.80, 95% confidence interval (CI): 0.69-0.93; P = 0.004) and the risk of intracerebral rebleeding (OR: 0.44, 95% CI: 0.26-0.74; P = 0.002) compared to craniotomy with no significant heterogeneity among the study results.
Conclusions: The present meta-analysis provides evidence that the stereotactic aspiration may be associated with a reduction in the odds of being dead or dependent in primary ICH, which should be interpreted with caution. Further trials are needed to identify those patients most likely to benefit from the stereotactic aspiration.
Conflict of interest statement
Figures




References
-
- van Asch CJ, Luitse MJ, Rinkel GJ, van der Tweel I, Algra A, et al. (2010) Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol 9: 167–176. - PubMed
-
- Sacco S, Marini C, Toni D, Olivieri L, Carolei A (2009) Incidence and 10-year survival of intracerebral hemorrhage in a population-based registry. Stroke 40: 394–399. - PubMed
-
- Adeoye O, Broderick JP (2010) Advances in the management of intracerebral hemorrhage. Nature Reviews Neurology 6: 593–601. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
