

Sulfonylurea treatment before genetic testing in neonatal diabetes: pros and cons
- PMID: 25238204
- PMCID: PMC4255121
- DOI: 10.1210/jc.2014-2494
Sulfonylurea treatment before genetic testing in neonatal diabetes: pros and cons
Abstract
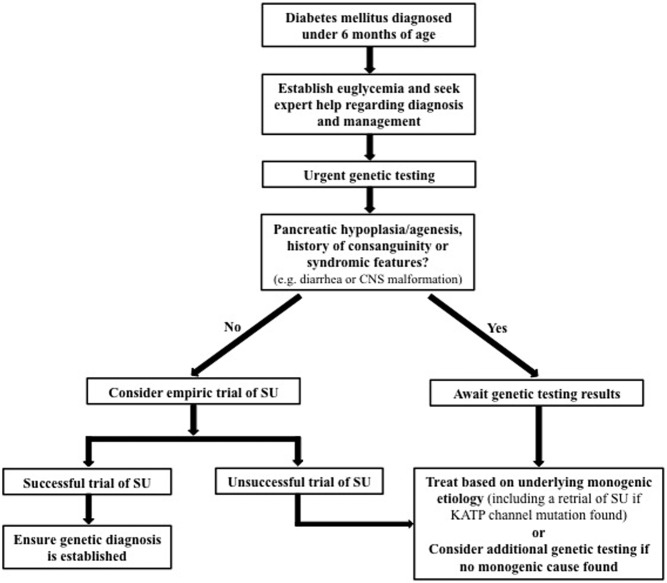
Context: Diabetes in neonates nearly always has a monogenic etiology. Earlier sulfonylurea therapy can improve glycemic control and potential neurodevelopmental outcomes in children with KCNJ11 or ABCC8 mutations, the most common gene causes.
Objective: Assess the risks and benefits of initiating sulfonylurea therapy before genetic testing results become available.
Design, setting, and patients: Observational retrospective study of subjects with neonatal diabetes within the University of Chicago Monogenic Diabetes Registry.
Main outcome measures: Response to sulfonylurea (determined by whether insulin could be discontinued) and treatment side effects in those treated empirically.
Results: A total of 154 subjects were diagnosed with diabetes before 6 months of age. A genetic diagnosis had been determined in 118 (77%), with 73 (47%) having a mutation in KCNJ11 or ABCC8. The median time from clinical diagnosis to genetic diagnosis was 10.4 weeks (range, 1.6 to 58.2 wk). In nine probands, an empiric sulfonylurea trial was initiated within 28 days of diabetes diagnosis. A genetic cause was subsequently found in eight cases, and insulin was discontinued within 14 days of sulfonylurea initiation in all of these cases.
Conclusions: Sulfonylurea therapy appears to be safe and often successful in neonatal diabetes patients before genetic testing results are available; however, larger numbers of cases must be studied. Given the potential beneficial effect on neurodevelopmental outcome, glycemic control, and the current barriers to expeditious acquisition of genetic testing, an empiric inpatient trial of sulfonylurea can be considered. However, obtaining a genetic diagnosis remains imperative to inform long-term management and prognosis.
Figures
Comment in
-
Letter to the editor: recent advances in genetic testing and treatment of neonatal diabetes mellitus.J Clin Endocrinol Metab. 2015 Jan;100(1):L13. doi: 10.1210/jc.2014-3808. J Clin Endocrinol Metab. 2015. PMID: 25559538 No abstract available.
-
Response letter to the editor.J Clin Endocrinol Metab. 2015 Jan;100(1):L14. doi: 10.1210/jc.2014-4089. J Clin Endocrinol Metab. 2015. PMID: 25559539 Free PMC article. No abstract available.
-
Letter to the Editor: Comments on "Sulfonylurea Treatment Before Genetic Testing in Neonatal Diabetes: Pros and Cons" by Carmody D, et al.J Clin Endocrinol Metab. 2016 Mar;101(3):L36. doi: 10.1210/jc.2015-4249. J Clin Endocrinol Metab. 2016. PMID: 26938375 No abstract available.
-
Response to the Letter to the Editor by Deeb A.J Clin Endocrinol Metab. 2016 Mar;101(3):L37. doi: 10.1210/jc.2016-1084. J Clin Endocrinol Metab. 2016. PMID: 26938376 No abstract available.
References
-
- Wiedemann B, Schober E, Waldhoer T, et al. Incidence of neonatal diabetes in Austria-calculation based on the Austrian Diabetes Register. Pediatr Diabetes. 2010;11:18–23. - PubMed
-
- Flanagan SE, Edghill EL, Gloyn AL, Ellard S, Hattersley AT. Mutations in KCNJ11, which encodes Kir6.2, are a common cause of diabetes diagnosed in the first 6 months of life, with the phenotype determined by genotype. Diabetologia. 2006;49:1190–1197. - PubMed
-
- Edghill EL, Dix RJ, Flanagan SE, et al. HLA genotyping supports a nonautoimmune etiology in patients diagnosed with diabetes under the age of 6 months. Diabetes. 2006;55:1895–1898. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
