

Facilitators and barriers to facility-based delivery in low- and middle-income countries: a qualitative evidence synthesis
- PMID: 25238684
- PMCID: PMC4247708
- DOI: 10.1186/1742-4755-11-71
Facilitators and barriers to facility-based delivery in low- and middle-income countries: a qualitative evidence synthesis
Abstract
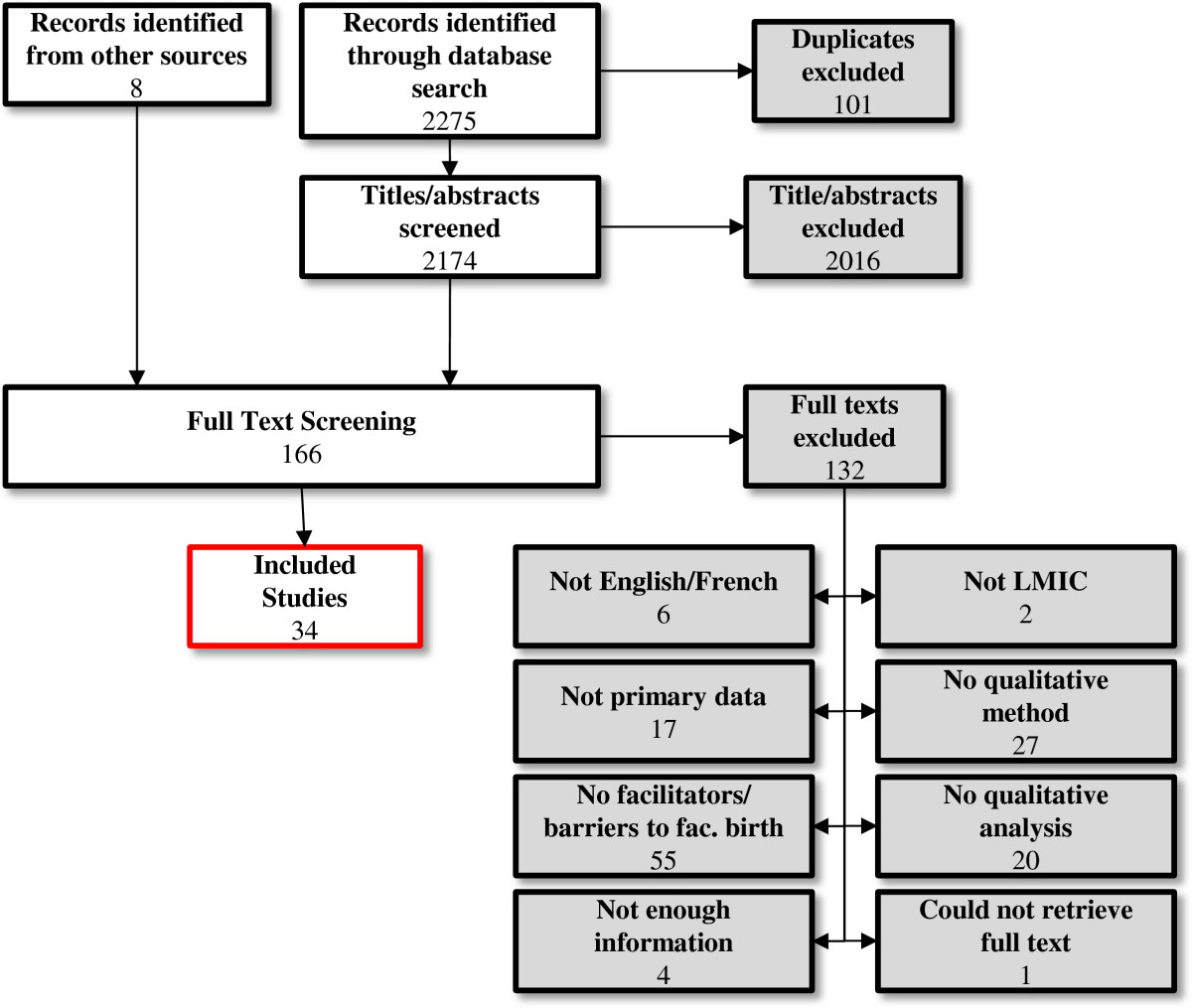
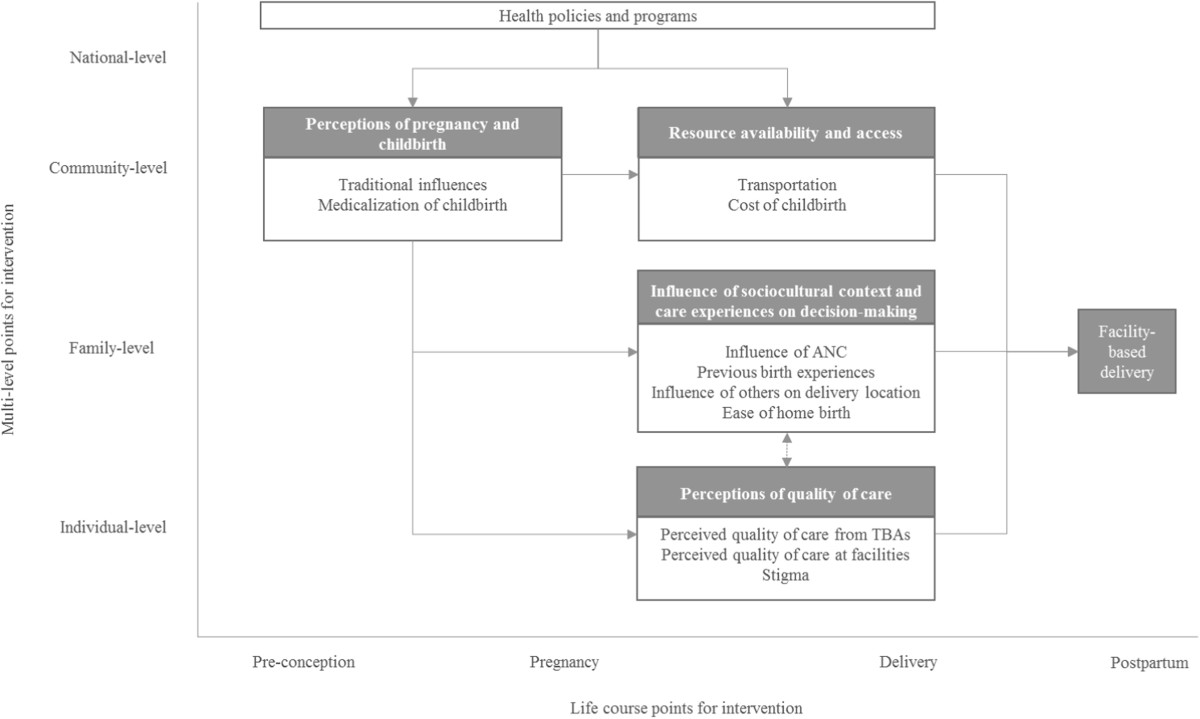
High-quality obstetric delivery in a health facility reduces maternal and perinatal morbidity and mortality. This systematic review synthesizes qualitative evidence related to the facilitators and barriers to delivering at health facilities in low- and middle-income countries. We aim to provide a useful framework for better understanding how various factors influence the decision-making process and the ultimate location of delivery at a facility or elsewhere. We conducted a qualitative evidence synthesis using a thematic analysis. Searches were conducted in PubMed, CINAHL and gray literature databases. Study quality was evaluated using the CASP checklist. The confidence in the findings was assessed using the CERQual method. Thirty-four studies from 17 countries were included. Findings were organized under four broad themes: (1) perceptions of pregnancy and childbirth; (2) influence of sociocultural context and care experiences; (3) resource availability and access; (4) perceptions of quality of care. Key barriers to facility-based delivery include traditional and familial influences, distance to the facility, cost of delivery, and low perceived quality of care and fear of discrimination during facility-based delivery. The emphasis placed on increasing facility-based deliveries by public health entities has led women and their families to believe that childbirth has become medicalized and dehumanized. When faced with the prospect of facility birth, women in low- and middle-income countries may fear various undesirable procedures, and may prefer to deliver at home with a traditional birth attendant. Given the abundant reports of disrespectful and abusive obstetric care highlighted by this synthesis, future research should focus on achieving respectful, non-abusive, and high-quality obstetric care for all women. Funding for this project was provided by The United States Agency for International Development (USAID) and the UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction, Department of Reproductive Health and Research, World Health Organization.
Figures
References
-
- World Health Organization . Trends in Maternal Mortality: 1990–2010. Geneva: WHO, UNICEF, UNFPA, & The World Bank; 2012.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
