

Early postoperative weight loss predicts maximal weight loss after sleeve gastrectomy and Roux-en-Y gastric bypass
- PMID: 25239175
- PMCID: PMC4422859
- DOI: 10.1007/s00464-014-3829-7
Early postoperative weight loss predicts maximal weight loss after sleeve gastrectomy and Roux-en-Y gastric bypass
Abstract
Background: Previous studies show that 'poor responders' to Roux-en-Y gastric bypass (RYGBP) may be identified on the basis of early postoperative weight loss. Early identification of poor responders could allow earlier provision of postoperative behavioural and/or intensive lifestyle interventions and enhance their maximal weight loss. Our aim was to investigate whether early postoperative weight loss predicts the maximal weight loss response after RYGBP and sleeve gastrectomy (SG).
Methods: We undertook a retrospective cross-sectional study of 1,456 adults who underwent either RYGBP (n = 918) or SG (n = 538) as a primary procedure in one of two European centres. Postoperative weight loss was expressed as weight loss velocity (WLV) and percentage weight loss. Linear regression analyses were performed to determine the association of early postoperative weight loss with maximal %WL, including adjustment for baseline variables.
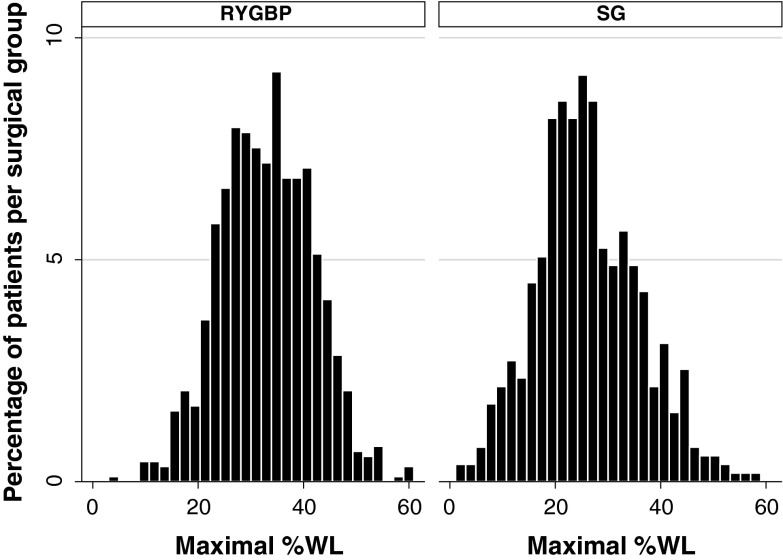
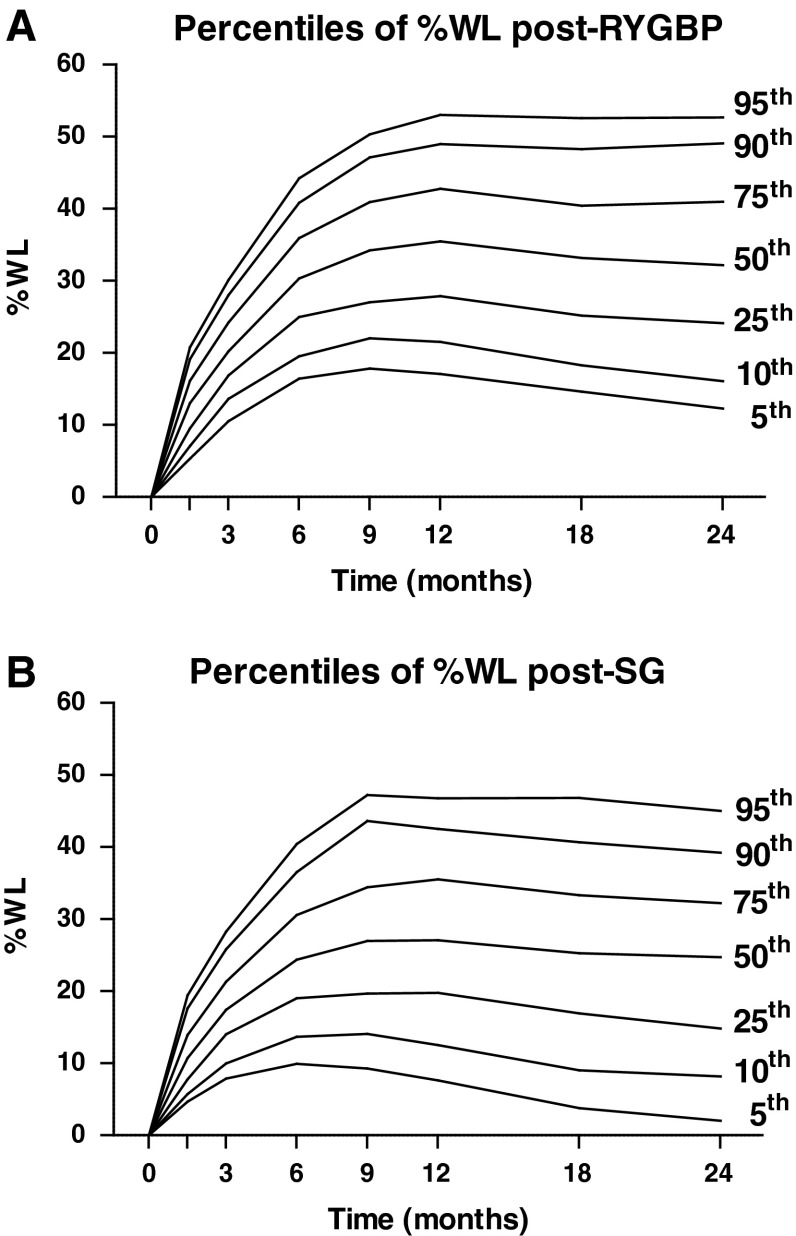
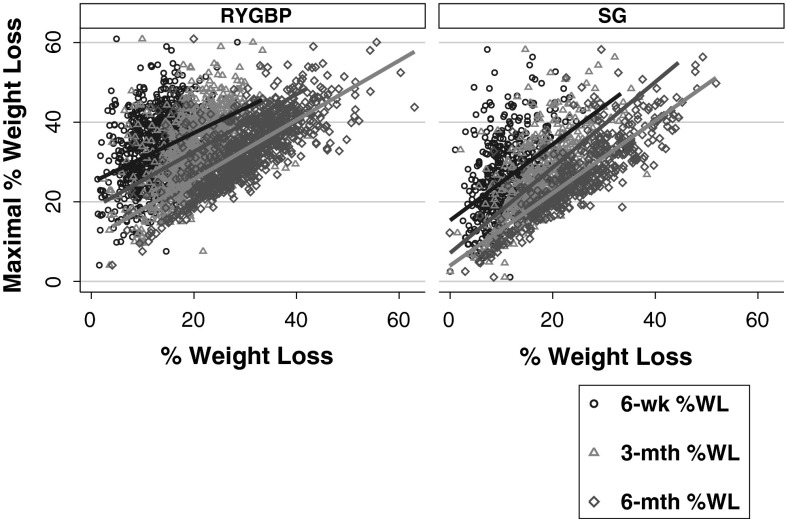
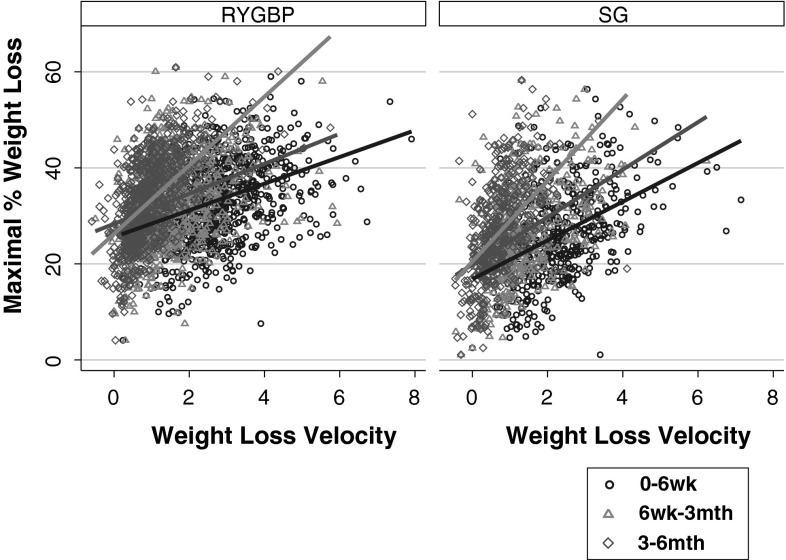
Results: There was marked variability in maximal %WL following both RYGBP (mean 32.9 %, range 4.1-60.9 %) and SG (mean 26.2 %, range 1.1-58.3 %). WLV 3-6 months postoperatively was more strongly associated with maximal %WL (r (2) = 0.32 for RYGBP and r (2) = 0.26 for SG, P < 0.001 for both) than either WLV 0-6 weeks or 6 weeks to 3 months postoperatively (r (2) = 0.14 and 0.10 for RYGBP, respectively; r (2) = 0.18 and 0.21 for SG, respectively; P < 0.001 for all). Multiple linear regression analysis, including baseline variables of age, sex, preoperative BMI, type 2 diabetes, ethnicity, and bariatric centre, revealed that 3-6 month WLV was an independent predictor of maximal %WL in both SG and RYGBP groups (standardised β-coefficients 0.51 and 0.52, respectively; P < 0.001 for both).
Conclusions: There is a marked variability in weight loss response following RYGBP and SG. Early postoperative weight loss can be used to identify patients whose predicted weight loss trajectories are suboptimal. Early targeting of poor responders with more intensive postoperative lifestyle and behavioural support could potentially enhance their weight loss response.
Figures
References
-
- Picot J et al (2009) The clinical effectiveness and cost-effectiveness of bariatric (weight loss) surgery for obesity: a systematic review and economic evaluation. Health Technol Assess 13(41):1–190, 215–357, iii–iv - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
