

Peripheral mechanisms in appetite regulation
- PMID: 25241326
- PMCID: PMC4369188
- DOI: 10.1053/j.gastro.2014.09.016
Peripheral mechanisms in appetite regulation
Abstract
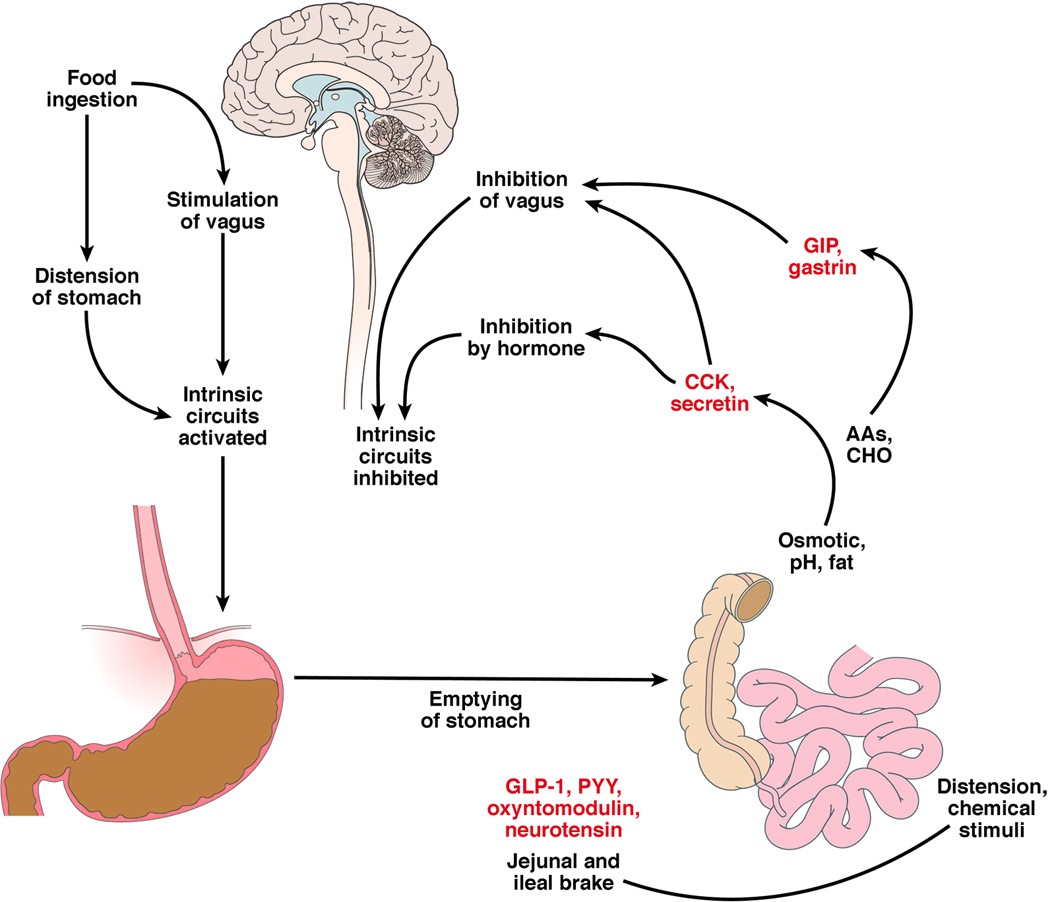
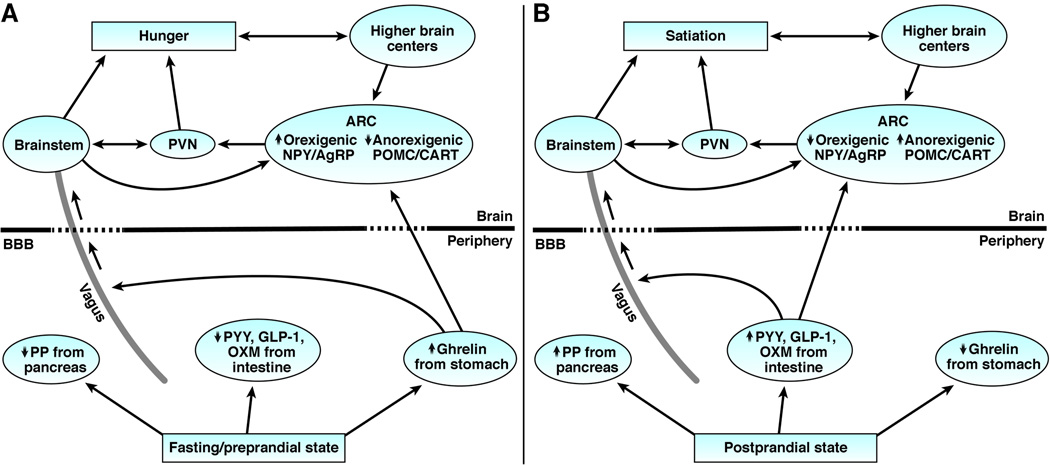
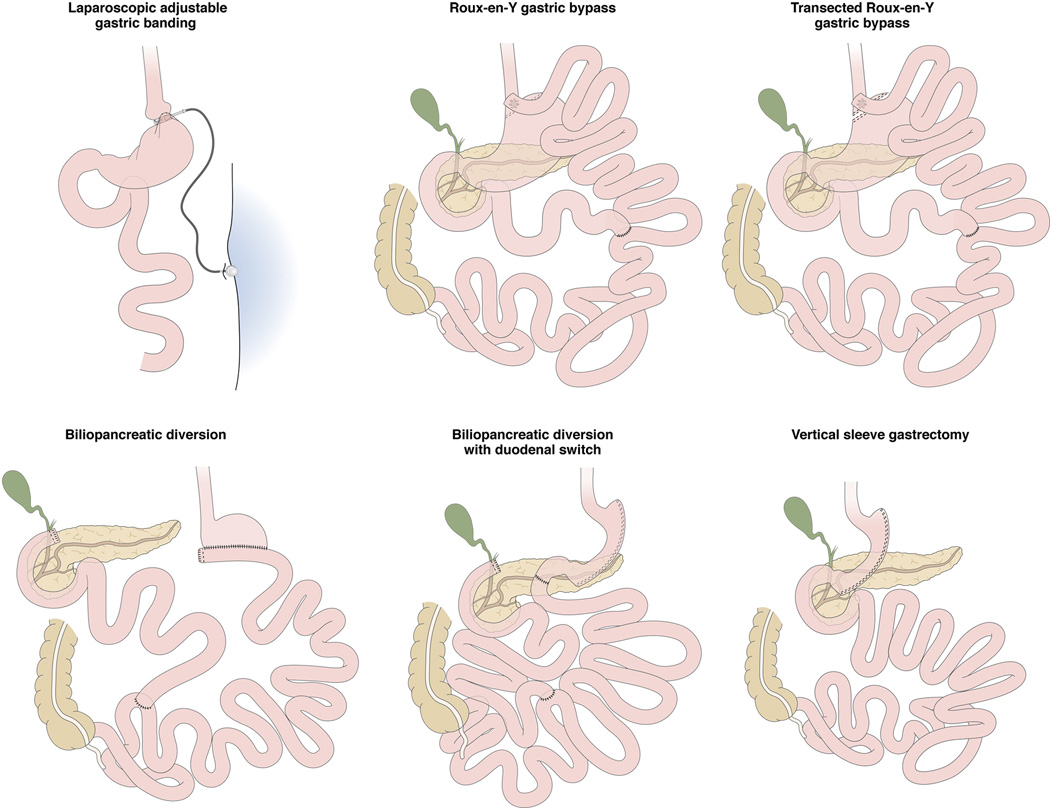
Peripheral mechanisms in appetite regulation include the motor functions of the stomach, such as the rate of emptying and accommodation, which convey symptoms of satiation to the brain. The rich repertoire of peripherally released peptides and hormones provides feedback from the arrival of nutrients in different regions of the gut from where they are released to exert effects on satiation, or regulate metabolism through their incretin effects. Ultimately, these peripheral factors provide input to the highly organized hypothalamic circuitry and vagal complex of nuclei to determine cessation of energy intake during meal ingestion, and the return of appetite and hunger after fasting. Understanding these mechanisms is key to the physiological control of feeding and the derangements that occur in obesity and their restoration with treatment (as shown by the effects of bariatric surgery).
Keywords: Neurohormonal; Satiation; Satiety; Stomach.
Copyright © 2015 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosures: No conflicts of interest related to the subject matter of this manuscript.
Figures

References
-
- Camilleri M. Integrated upper gastrointestinal response to food intake. Gastroenterology. 2006;131:640–658. - PubMed
-
- Csendes A, Burgos AM. Size, volume and weight of the stomach in patients with morbid obesity compared to controls. Obes Surg. 2005;15:1133–1136. - PubMed
-
- Tack J, Bisschops R. Mechanisms underlying meal-induced symptoms in functional dyspepsia. Gastroenterology. 2004;127:1844–1847. - PubMed
-
- Feinle-Bisset C, Horowitz M. Dietary factors in functional dyspepsia. Neurogastroenterol Motil. 2006;18:608–618. - PubMed
-
- Delgado-Aros S, Camilleri M, Castillo EJ, et al. Effect of gastric volume or emptying on meal-related symptoms after liquid nutrients in obesity: a pharmacologic study. Clin Gastroenterol Hepatol. 2005;3:997–1006. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
