

Pathogenesis of Osteoporosis
- PMID: 25243055
- PMCID: PMC4167368
- DOI: 10.1210/TEAM.9781879225718.ch2
Pathogenesis of Osteoporosis
Abstract
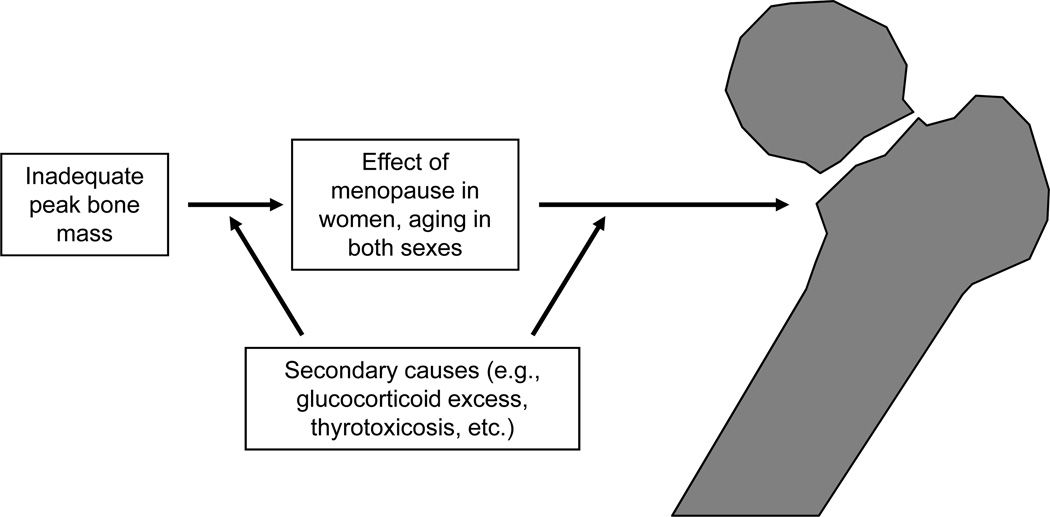
As for most multifactorial disorders, the pathogenesis of osteoporosis is complex, and a different set of mechanisms may be operative in any given individual. However, there are certain common causes of bone loss and increased fracture risk with aging in most people. These include genetic factors contributing to the acquisition of peak bone mass, illnesses affecting skeletal growth and development, sex steroid deficiency following the menopause in women and with aging in men, and intrinsic, age-related changes in bone metabolism. Superimposed on these factors are specific secondary causes of bone loss, such as corticosteroid use or other illnesses affecting bone metabolism that may contribute to fracture risk in individuals exposed to these factors. The past decade has witnessed tremendous advances in our understanding of each of these various causes of bone loss, leading to the development of novel, mechanism-based therapeutic approaches to prevent and treat this important public health disorder.
Keywords: bone loss; fractures; osteoporosis.
Figures
References
-
- Riggs BL, Khosla S, Melton LJ. Sex steroids and the construction and conservation of the adult skeleton. Endocr Rev. 2002;23:279–302. - PubMed
-
- Khosla S, Melton LJ, Riggs BL. Estrogen and the male skeleton. J Clin Endocrinol Metab. 2002;87:1443–1450. - PubMed
-
- Cooper C, Eriksson JG, Forsen T, Osmond C, Tuomilehto J, Barker DJP. Maternal height, childhood growth and risk of hip fracture in later life: a longitudinal study. Osteoporos Int. 2001;12:623–629. - PubMed
-
- Barker DJ. The Wellcome Foundation Lecture, 1994. The fetal origins of adult disease. Proc Biol Sci. 1995;262:37–43. - PubMed
-
- Dennison EM, Syddall HE, Sayer AA, Gilbody HJ, Cooper C. Birth weight and weight at 1 year are independent determinants of bone mass in the seventh decade: the Hertfordshire cohort study. Pediatr Res. 2005;57:582–586. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous