

Ocular outcomes evaluation in a 14-day head-down bed rest study
- PMID: 25245897
- PMCID: PMC4240225
- DOI: 10.3357/ASEM.4055.2014
Ocular outcomes evaluation in a 14-day head-down bed rest study
Abstract
Introduction: We evaluated ocular outcomes in a 14-d head-down tilt (HDT) bed rest (BR) study designed to simulate the effects of microgravity on the human body.
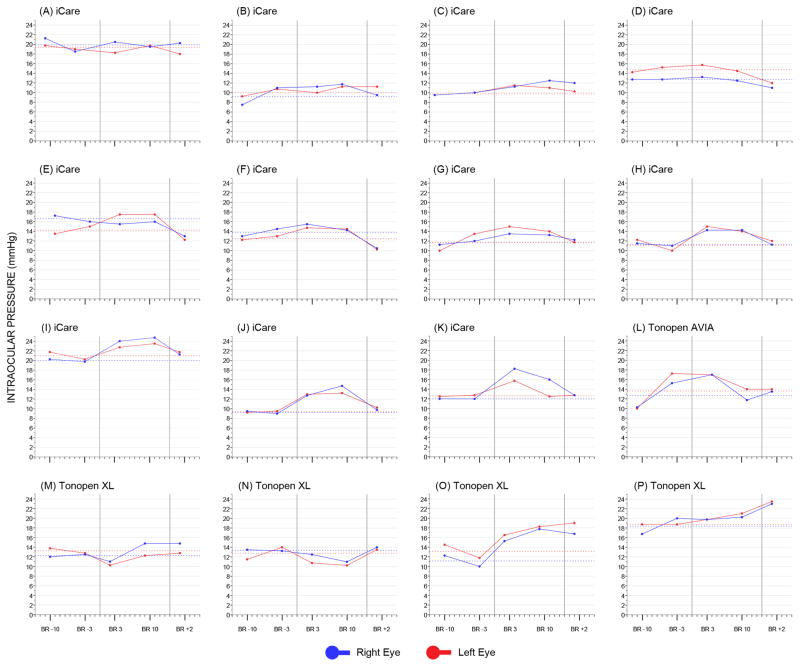
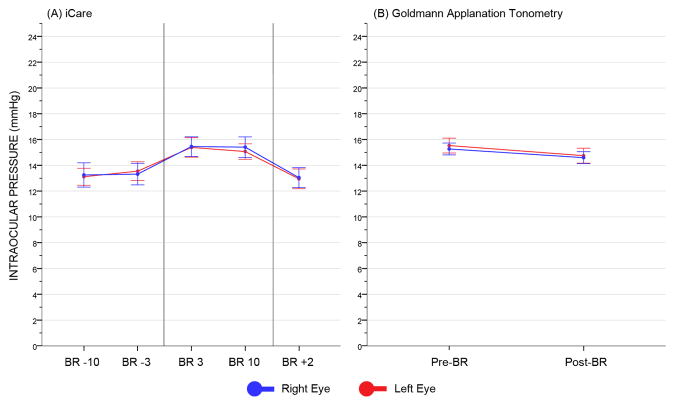
Methods: Healthy subjects were selected using NASA standard screening procedures. Standardized NASA BR conditions were implemented (e.g., strict sleep-wake cycle, standardized diet, 24-hour-a-day BR, continuous video monitoring). Subjects maintained a 6° HDT position for 14 consecutive days. Weekly ophthalmological examinations were performed in the sitting (pre/post-BR) and HDT (in-bed phase) positions. Equivalency tests with optimal-alpha techniques evaluated pre/post-BR differences in best-corrected visual acuity (BCVA), spherical equivalent, intraocular pressure (IOP), Spectral-domain OCT retinal nerve fiber layer thickness (RNFLT), optic disc and macular parameters.
Results: 16 subjects (12 men and 4 women) were enrolled. Nearly all ocular outcomes were within our predefined clinically relevant thresholds following HDTBR, except near BCVA (pre/post-BR mean difference: -0.06 logMAR), spherical equivalent (-0.30 D), Tonopen XL IOP (+3.03 mmHg) and Spectralis OCT average (+1.14 μm), temporal-inferior (+1.58 μm) and nasal-inferior RNFLT (+3.48 μm). Modified Amsler grid, red dot test, confrontational visual field, and color vision were within normal limits throughout. No changes were detected on stereoscopic color fundus photography.
Discussion: A few functional and structural changes were detected after 14-d HDTBR, notably an improved BCVA possibly due to learning effect and RNFL thickening without signs of optic disc edema. In general, 6° HDTBR determined a small nonprogressive IOP elevation, which returned to baseline levels post-BR. Further studies with different BR duration and/or tilt angle are warranted to investigate microgravity-induced ophthalmological changes.
Figures
References
-
- Awad H, Santilli S, Ohr M, Roth A, Yan W, et al. The effects of steep trendelenburg positioning on intraocular pressure during robotic radical prostatectomy. Anesth Analg. 2009;109:473–8. - PubMed
-
- Berdahl JP, Allingham RR. Intracranial pressure and glaucoma. Curr Opin Ophthalmol. 2010;21:106–11. - PubMed
-
- Borahay MA, Patel PR, Walsh TM, Tarnal V, Koutrouvelis A, et al. Intraocular pressure and steep Trendelenburg during minimally invasive gynecologic surgery: is there a risk? J Minim Invasive Gynecol. 2013;20:819–24. - PubMed
-
- Garcia-Martin E, Pinilla I, Idoipe M, Fuertes I, Pueyo V. Intra and interoperator reproducibility of retinal nerve fibre and macular thickness measurements using Cirrus Fourier-domain OCT. Acta Ophthalmol. 2011;89:e23–9. - PubMed
-
- Garway-Heath DF, Kotecha A, Lerner F, Dayanir V, Brandt JD, et al. Measurement of intraocular pressure. In: Weinreb RN, Brandt JD, Garway-Heath DF, Medeiros FA, editors. Intraocular pressure: reports and consensus statements of the 4th global AIGS consensus meeting on intraocular pressure. The Hague, The Netherlands: Kugler Publications; 2007. p. 31.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources