

Brain metastases in gastrointestinal cancers: is there a role for surgery?
- PMID: 25247579
- PMCID: PMC4200819
- DOI: 10.3390/ijms150916816
Brain metastases in gastrointestinal cancers: is there a role for surgery?
Abstract
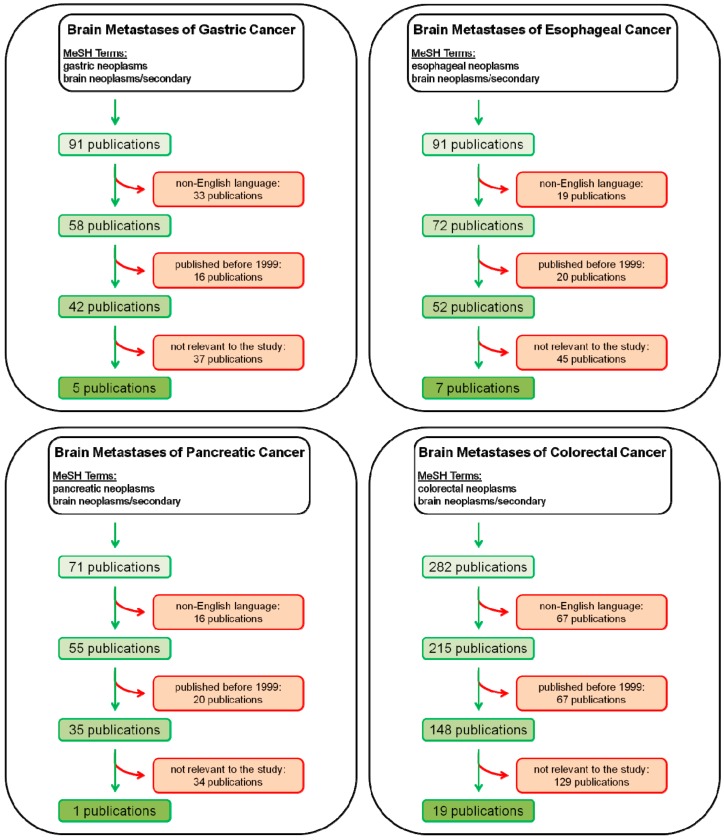
About 10% of all cancer patients will develop brain metastases during advanced disease progression. Interestingly, the vast majority of brain metastases occur in only three types of cancer: Melanoma, lung and breast cancer. In this review, we focus on summarizing the prognosis and impact of surgical resection of brain metastases originating from gastrointestinal cancers such as esophageal, gastric, pancreatic and colorectal cancer. The incidence of brain metastases is <1% in pancreatic and gastric cancer and <4% in esophageal and colorectal cancer. Overall, prognosis of these patients is very poor with a median survival in the range of only months. Interestingly, a substantial number of patients who had received surgical resection of brain metastases showed prolonged survival. However, it should be taken into account that all these studies were not randomized and it is likely that patients selected for surgical treatment presented with other important prognostic factors such as solitary brain metastases and exclusion of extra-cranial disease. Nevertheless, other reports have demonstrated long-term survival of patients upon resection of brain metastases originating from gastrointestinal cancers. Thus, it appears to be justified to consider aggressive surgical approaches for these patients.
Figures
References
-
- Jemal A., Bray F., Center M.M., Ferlay J., Ward E., Forman D. Global cancer statistics. CA Cancer J. Clin. 2010;61:69–90. - PubMed
-
- Wan L., Pantel K., Kang Y. Tumor metastasis: Moving new biological insights into the clinic. Nat. Med. 2013;19:1450–1464. - PubMed
-
- Gavrilovic I.T., Posner J.B. Brain metastases: Epidemiology and pathophysiology. J. Neuro-Oncol. 2005;75:5–14. - PubMed
-
- Barnholtz-Sloan J.S., Sloan A.E., Davis F.G., Vigneau F.D., Lai P., Sawaya R.E. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J. Clin. Oncol. 2004;22:2865–2872. - PubMed
-
- Nayak L., Lee E.Q., Wen P.Y. Epidemiology of brain metastases. Curr. Oncol. Rep. 2012;14:48–54. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
