

Management of severe hyponatremia: infusion of hypertonic saline and desmopressin or infusion of vasopressin inhibitors?
- PMID: 25247759
- PMCID: PMC4206391
- DOI: 10.1097/MAJ.0000000000000331
Management of severe hyponatremia: infusion of hypertonic saline and desmopressin or infusion of vasopressin inhibitors?
Abstract
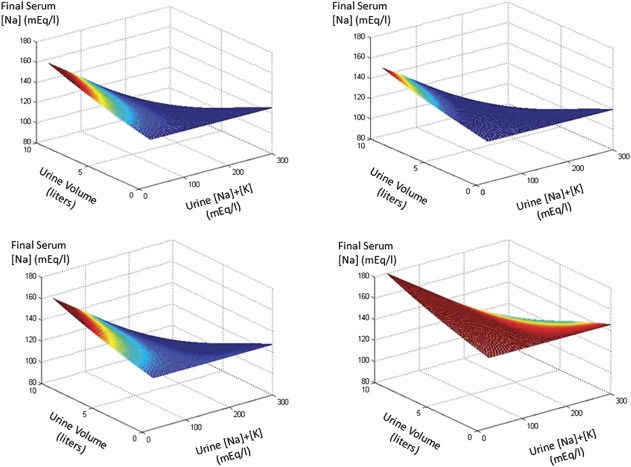
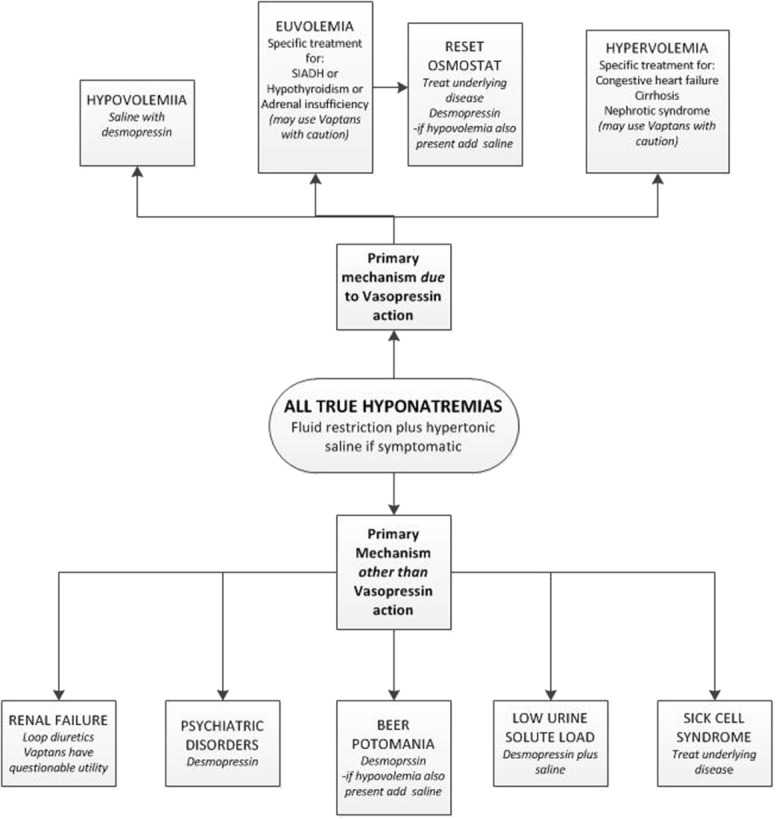
Rapid correction of severe hyponatremia carries the risk of osmotic demyelination. Two recently introduced methods of correction of hyponatremia have diametrically opposite effects on aquaresis. Inhibitors of vasopressin V2 receptor (vaptans) lead to the production of dilute urine, whereas infusion of desmopressin causes urinary concentration. Identification of the category of hyponatremia that will benefit from one or the other treatment is critical. In general, vaptans are effective in hyponatremias presenting with concentrated urine and, with the exception of hypovolemic hyponatremia, can be used as their primary treatment. Desmopressin is effective in hyponatremias presenting with dilute urine or developing urinary dilution after saline infusion. In this setting, desmopressin infusion helps prevent overcorrection of the hyponatremia. Monitoring of the changes in serum sodium concentration as a guide to treatment changes is imperative regardless of the initial treatment of severe hyponatremia.
Conflict of interest statement
The authors have no financial or other conflicts of interest to disclose.
Figures
References
-
- Lien YH. Are we ignoring dysnatremia? Am J Med 2012;125:1045–6 - PubMed
-
- Kokko JP. Symptomatic hyponatremia with hypoxia is a medical emergency. Kidney Int 2006;69:1291–3 - PubMed
-
- Sterns RH, Hix JK, Silver S. Treatment of hyponatremia. Curr Opin Nephrol Hypertens 2010;19:493–8 - PubMed
-
- Sonnenblick M, Friedlander Y, Rosin AJ. Diuretic-induced severe hyponatremia. Review and analysis of 129 reported patients. Chest 1993;103:601–6 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
