

A nurse-led up-titration clinic improves chronic heart failure optimization of beta-adrenergic receptor blocking therapy--a randomized controlled trial
- PMID: 25248944
- PMCID: PMC4182807
- DOI: 10.1186/1756-0500-7-668
A nurse-led up-titration clinic improves chronic heart failure optimization of beta-adrenergic receptor blocking therapy--a randomized controlled trial
Abstract
Background: Beta-adrenergic blockade has been shown to improve left ventricular function, reduce hospital admissions and improve survival in chronic heart failure with reduced ejection fraction (HFrEF), with mortality reduction starting early after beta-adrenergic receptor blocker initiation and being dose-related. The aim of this pilot study was to determine the effectiveness of a nurse-led titration clinic in improving the time required for patients to reach optimal doses of the beta-adrenergic receptor blocking agents.
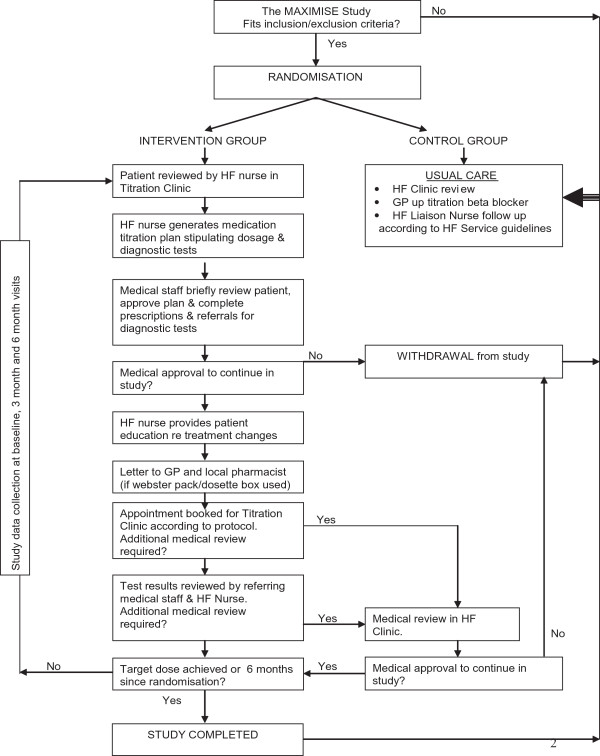
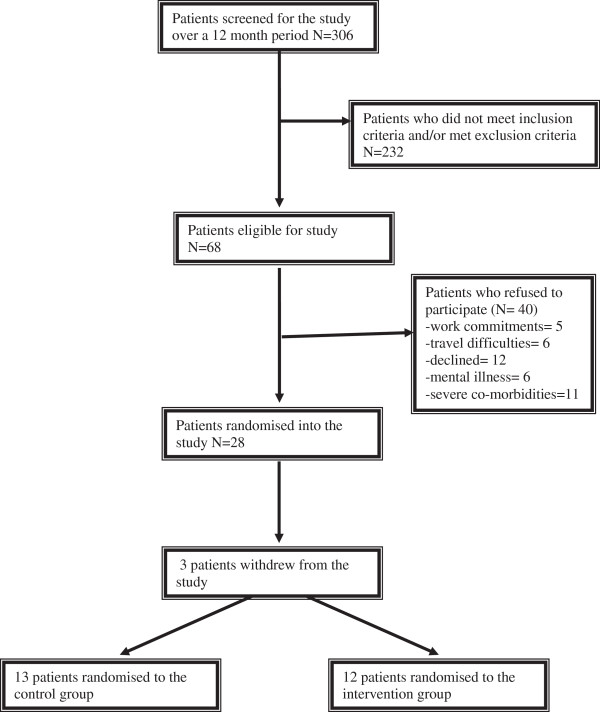
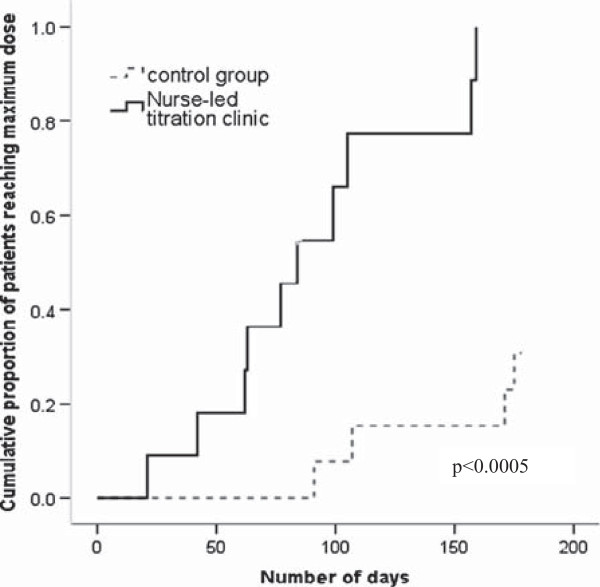
Method: We conducted a prospective pilot randomized controlled trial. Twenty eight patients with CHF were randomized to optimisation of beta-adrenergic receptor blocker therapy over six months by either a nurse-led titration (NLT) clinic, led by a nurse specialist with the support of a cardiologist in a CHF clinic, or by their primary care physician (usual care (UC)). The primary endpoint was time to maximal beta-adrenergic receptor blocker dose. The secondary end-point was the proportion of patients reaching the target dose of beta-adrenergic receptor blocker by six months.
Results: The patients were predominantly men (72%), age 67 ± 16 years; New York Heart Association (NYHA) functional class I (32%), II (44%) and III (20%); baseline left ventricular ejection fraction 33 ± 10%, and a low mean Charlson co-morbidity score of 2.5 ± 1.4. The time to maximum dose was shorter in the NLT group compared to the UC group (90 ± 14 vs 166 ± 8 days, p < 0.0005). At six months, in the NLT group there were nine patients (82%) on high dose and one patient (9%) on low dose beta-adrenergic receptor blocker compared to the UC group with five (42%) patients reaching maximum dose and five (42%) patients on low dose (p = 0.04). The patients allocated to the NLT group also had significantly less worsening of depression between baseline and six months (p = 0.006).
Conclusion: A NLT clinic improves optimisation of beta-adrenergic receptor blocker therapy through increasing the proportion of patients reaching maximal dose and facilitating rapid up-titration of beta-adrenergic receptor blocker agents in patients with chronic HFrEF.
Trial registration: Australian Clinical Trials Registry (ACTRN012606000383561).
Figures
References
-
- Jhund PS, MacIntyre K, Simpson CR, Lewsey JD, Stewart S, Redpath A, Chalmers JWT, Capewell S, McMurray JJV. Long-term trends in first hospitalisation for heart failure and subsequent survival between 1986 and 2003. A population study of 5.1 million people. Circulation. 2009;119:515–523. doi: 10.1161/CIRCULATIONAHA.108.812172. - DOI - PubMed
-
- Bleumink GS, Knetsch AM, Sturkenboom MCJM, Straus SM, Hofman A, Deckers JW, Witteman JCM, Stricker BH. Quantifying the heart failure epidemic: prevalence, incidence rate, lifetime risk and prognosis of heart failure. The Rotterdam Study. Eur Heart J. 2004;25(18):1614–1619. doi: 10.1016/j.ehj.2004.06.038. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
