

Silicone oil pupil block glaucoma in a pseudophakic eye
- PMID: 25249219
- PMCID: PMC4173143
- DOI: 10.1136/bcr-2014-205018
Silicone oil pupil block glaucoma in a pseudophakic eye
Abstract
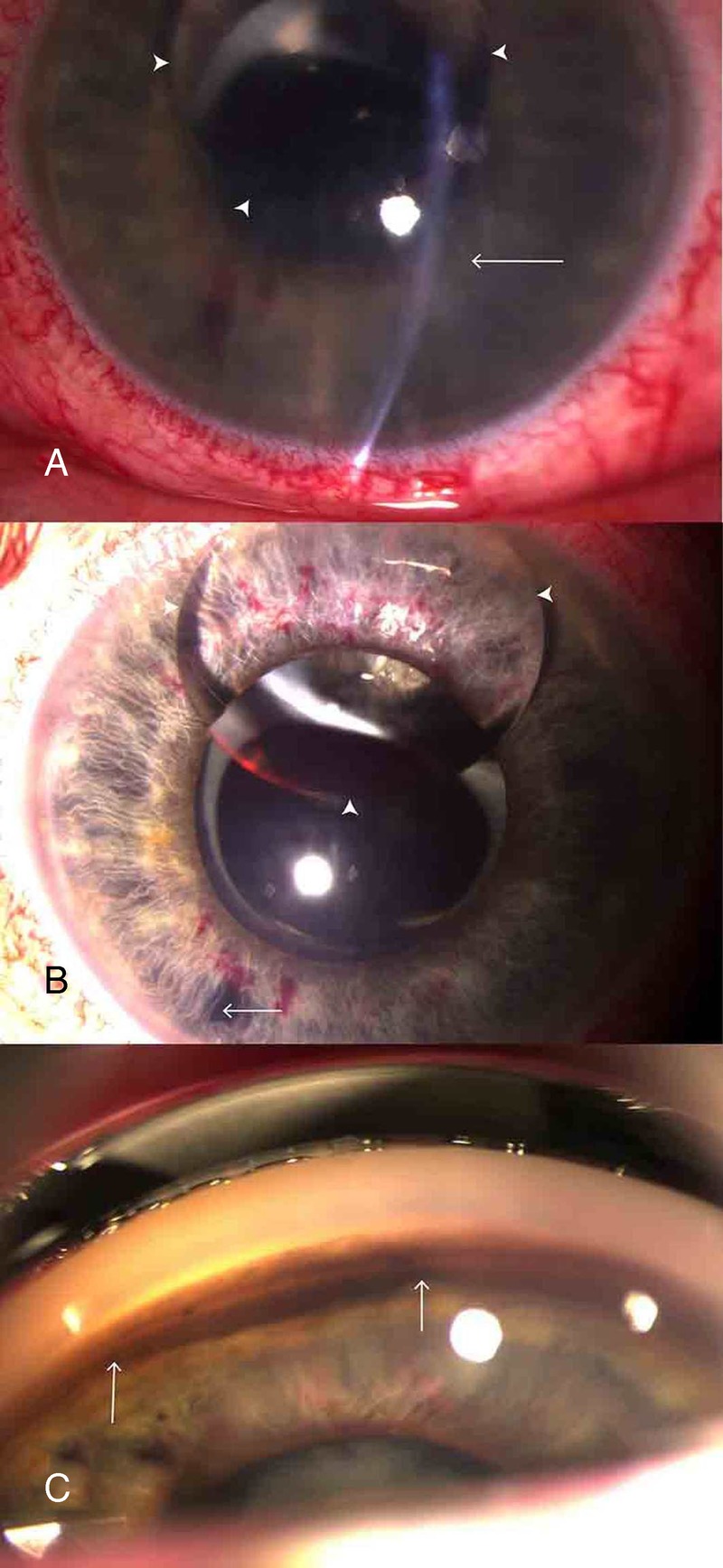
Intravitreal silicone oil achieves an effective endotamponade in patients with complex retinal detachments. Silicone oil displacement into the anterior chamber risks glaucoma and endothelial failure. We describe a 52-year-old patient with pseudophakia with silicone oil endotamponade presenting with visual loss and intraocular pressure of 60 mm Hg. Inferior YAG iridotomy was undertaken to repatriate silicone oil to the posterior segment. Despite normal intraocular pressure, acute corneal oedema occurred postiridotomy, resolving spontaneously over 2 weeks. Pupil block glaucoma secondary to silicone oil requires a management approach based on an understanding of silicone oil fluidics. Careful selection of inferior laser iridotomy site is critical to effectively reverse pupil block. Anterior migration of silicone oil in patients with pseudophakia is rare. We offer an hypothesis to explain unanticipated transient corneal oedema following silicone oil displacement from the anterior chamber. Clinicians must discuss the possibility of transient or permanent endothelial failure preoperatively in this patient group.
2014 BMJ Publishing Group Ltd.
Figures

References
-
- Riedel KG, Gabel VP, Neubauer L, et al. . Intravitreal silicone oil injection: complications and treatment of 415 consecutive patients. Graefes Arch Clin Exp Ophthalmol 1990;228:19–23 - PubMed
-
- Nakamura K, Refojo MF, Crabtree DV, et al. . Ocular toxicity of low-molecular-weight components of silicone and fluorosilicone oils. Invest Ophthalmol Vis Sci 1991;32:3007–20 - PubMed
-
- Merriman MB, Vote B, McGeorge A. Silicone oil pupil-block acute angle-closure glaucoma: optimal laser position. Retina 2003;23:407–9 - PubMed
-
- Joussen AM, Rizzo S, Kirchhof B, et al. . Heavy silicone oil versus standard silicone oil in as vitreous tamponade in inferior PVR (HSO Study): interim analysis. Acta Ophthalmol 2011;89:e483–9 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical