

Factors associated with periesophageal vagal nerve injury after pulmonary vein antrum isolation
- PMID: 25249299
- PMCID: PMC4323793
- DOI: 10.1161/JAHA.114.001209
Factors associated with periesophageal vagal nerve injury after pulmonary vein antrum isolation
Abstract
Background: Periesophageal vagal nerve injury is recognized as a rare complication in atrial fibrillation ablation procedures. We investigated the factors associated with the occurrence of symptomatic periesophageal vagal nerve injury after pulmonary vein antrum isolation.
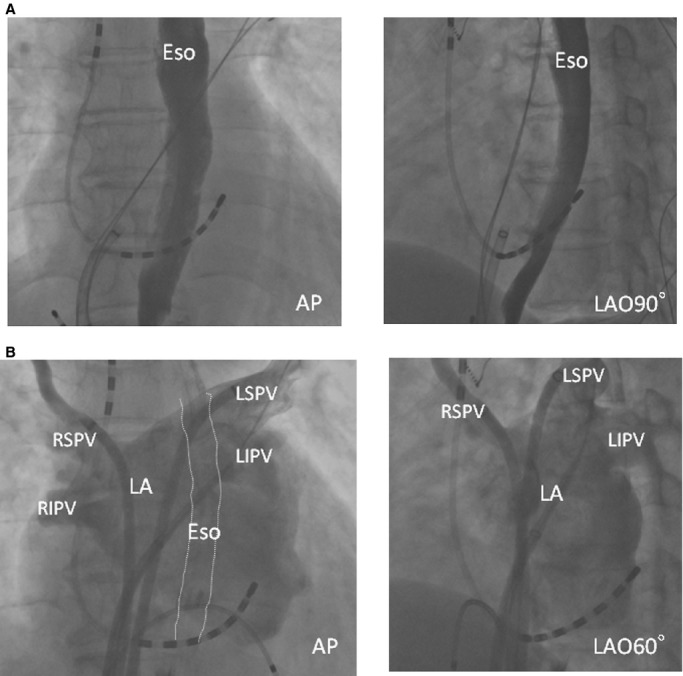
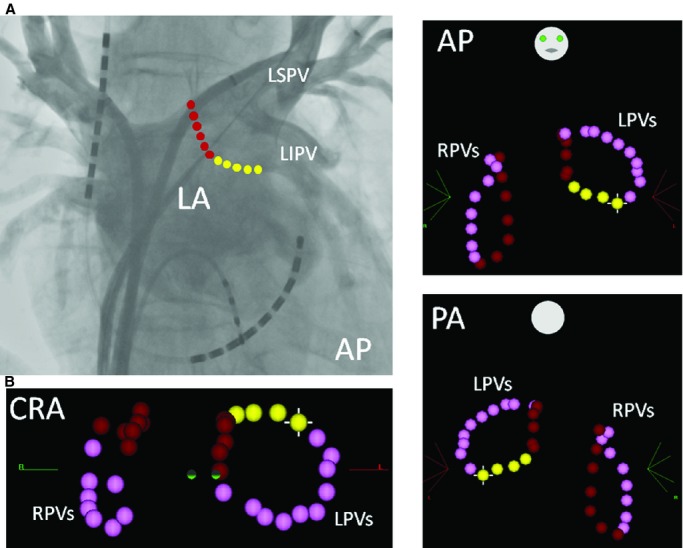
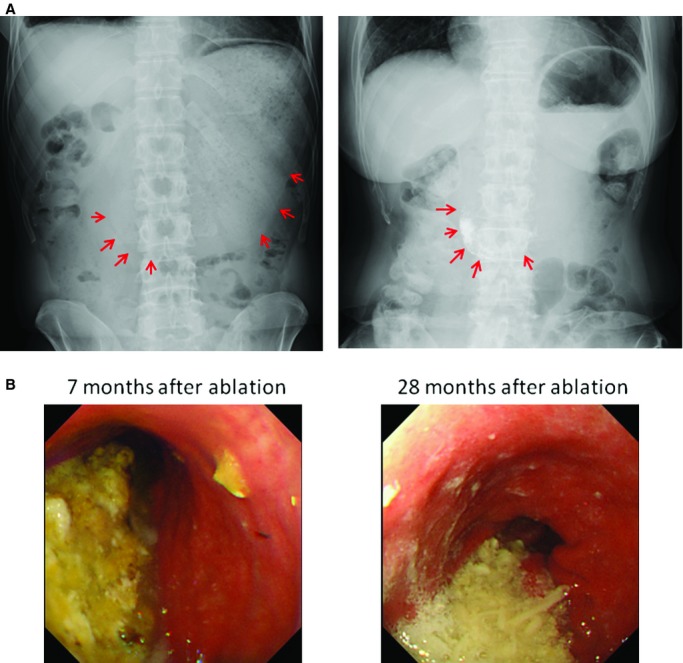
Methods and results: Overall, 535 consecutive patients who underwent sole pulmonary vein antrum isolation were included. Point-by-point radiofrequency applications were applied using irrigated-tip catheters under minimal sedation without esophageal temperature monitoring. In the initial 165 patients, the ablation settings for the posterior left atrium were a maximum energy of 25 to 30 W and a duration of 30 seconds. In the subsequent 370 patients, the power was additionally limited to 20 to 25 W at specific parts of the posterior left atrium where the ablation line transversed the esophagus. Symptomatic gastric hypomotility was found in 13 patients, and all were observed during the initial period (7.9%). No other collateral damage was observed. Logistic regression analysis revealed that the body mass index was the only independent predictor for identifying patients with gastric hypomotility (odds ratio 0.770; 95% confidence interval 0.643 to 0.922; P=0.0045) during the initial period. The prevalence of gastric hypomotility was significantly higher in the initial study period than subsequently (0 of 370, 0%; P<0.0001). All except for 1 patient recovered completely with conservative treatment within 4 months after the procedure.
Conclusions: Periesophageal vagal nerve injury is more common collateral damage than direct esophageal injury in pulmonary vein antrum isolation procedures. Titrating the radiofrequency energy at specific areas where the ablation line transverses the esophagus and taking account of the body mass index might reduce occurrences not only of direct esophageal damage but also of periesophageal vagal nerve injury in pulmonary vein antrum isolation procedures.
Keywords: atrial fibrillation; catheter ablation; collateral damage; complication; periesophageal vagal nerve injury; pulmonary vein isolation.
© 2014 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures

References
-
- Haïssaguerre M, Jaïs P, Shah DC, Takahashi A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Métayer P, Clémenty J. Spontaneous initiation of atrial fibrillation by ectopic beats originating from the pulmonary veins. N Engl J Med. 1998; 339:659-666. - PubMed
-
- Nault I, Miyazaki S, Forclaz A, Wright M, Jadidi A, Jaïs P, Hocini M, Haïssaguerre M. Drugs vs. ablation for the treatment of atrial fibrillation: the evidence supporting catheter ablation. Eur Heart J. 2010; 31:1046-1054. - PubMed
-
- Takahashi A, Iesaka Y, Takahashi Y, Takahashi R, Kobayashi K, Takagi K, Kuboyama O, Nishimori T, Takei H, Amemiya H, Fujiwara H, Hiraoka M. Electrical connections between pulmonary veins: implication for ostial ablation of pulmonary veins in patients with paroxysmal atrial fibrillation. Circulation. 2002; 105:2998-3003. - PubMed
-
- Liu X, Dong J, Mavrakis HE, Hu F, Long D, Fang D, Yu R, Tang R, Hao P, Lu C, He X, Liu X, Vardas PE, Ma C. Achievement of pulmonary vein isolation in patients undergoing circumferential pulmonary vein ablation: a randomized comparison between two different isolation approaches. J Cardiovasc Electrophysiol. 2006; 17:1263-1270. - PubMed
-
- Arentz T, Weber R, Bürkle G, Herrera C, Blum T, Stockinger J, Minners J, Neumann FJ, Kalusche D. Small and large isolation areas around the pulmonary veins for treatment of atrial fibrillation? Results from a prospective randomized study. Circulation. 2007; 115:3057-3063. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
