Pituitary stalk interruption syndrome: Case report of three cases with review of literature
- PMID: 25250085
- PMCID: PMC4166852
- DOI: 10.4103/1817-1745.139363
Pituitary stalk interruption syndrome: Case report of three cases with review of literature
Abstract
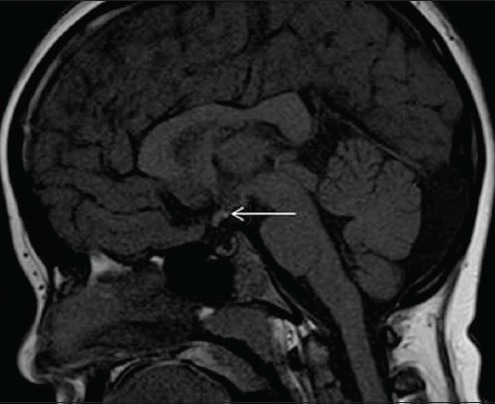
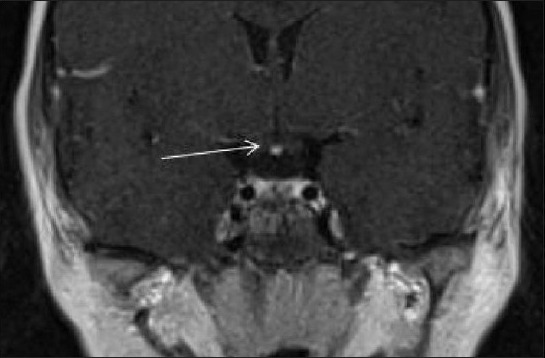
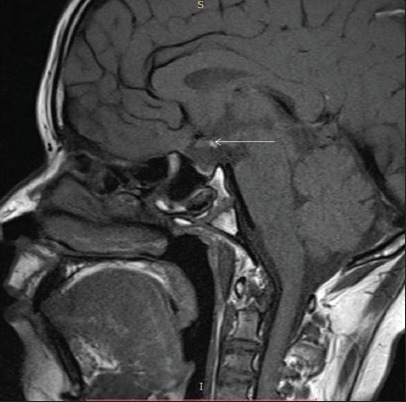
Pickardt syndrome (Pickardt-Fahlbusch syndrome) is a rare congenital syndrome characterized by tertiary hypothyroidism caused by the interruption of the portal veins between hypothalamus and adenohypophysis. Typical features of this syndrome are tertiary hypothyroidism with low thyroid stimulating hormone, hyperprolactinemia and other pituitary hormone deficiencies. Pituitary stalk interruption syndrome is characterized by a triad of thin or interrupted pituitary stalk, aplasia or hypoplasia of the anterior pituitary and absent or ectopic posterior pituitary (EPP) seen on magnetic resonance imaging (MRI). It is a congenital anomaly of pituitary whose exact prevalence is unknown. In some cases, it is restricted to EPP or pituitary stalk interruption. We are presenting the case history along with MRI finding of three children's who presented with short stature and delayed puberty.
Keywords: Delayed puberty; ectopic posterior pituitary; multiple pituitary hormones deficiency; pituitary stalk interruption syndrome.
Conflict of interest statement
Figures



References
-
- El Chehadeh-Djebbar S, Callier P, Masurel-Paulet A, Bensignor C, Méjean N, Payet M, et al. 17q21.31 microdeletion in a patient with pituitary stalk interruption syndrome. Eur J Med Genet. 2011;54:369–73. - PubMed
-
- Simmons GE, Suchnicki JE, Rak KM, Damiano TR. MR imaging of the pituitary stalk: Size, shape, and enhancement pattern. AJR Am J Roentgenol. 1992;159:375–7. - PubMed
-
- Tauber M, Chevrel J, Diene G, Moulin P, Jouret B, Oliver I, et al. Long-term evolution of endocrine disorders and effect of GH therapy in 35 patients with pituitary stalk interruption syndrome. Horm Res. 2005;64:266–73. - PubMed
-
- Pinto G, Netchine I, Sobrier ML, Brunelle F, Souberbielle JC, Brauner R. Pituitary stalk interruption syndrome: A clinical-biological-genetic assessment of its pathogenesis. J Clin Endocrinol Metab. 1997;82:3450–4. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources