

Extra-renal manifestations of complement-mediated thrombotic microangiopathies
- PMID: 25250305
- PMCID: PMC4157546
- DOI: 10.3389/fped.2014.00097
Extra-renal manifestations of complement-mediated thrombotic microangiopathies
Abstract
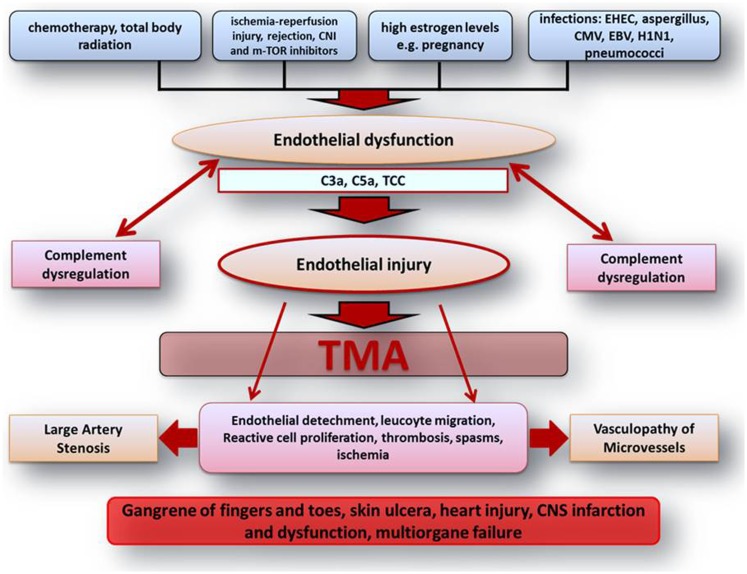
Thrombotic microangiopathies (TMA) are rare but severe disorders, characterized by endothelial cell activation and thrombus formation leading to hemolytic anemia, thrombocytopenia, and organ failure. Complement over activation in combination with defects in its regulation is described in an increasing number of TMA and if primary for the disease denominated as atypical hemolytic-uremic syndrome. Although TMA predominantly affects the renal microvasculature, extra-renal manifestations are observed in 20% of patients including involvement of the central nerve system, cardiovascular system, lungs, skin, skeletal muscle, and gastrointestinal tract. Prompt diagnosis and treatment initiation are therefore crucial for the prognosis of disease acute phase and the long-term outcome. This review summarizes the available evidence on extra-renal TMA manifestations and discusses the role of acute and chronic complement activation by highlighting its complex interaction with inflammation, coagulation, and endothelial homeostasis.
Keywords: TMA; aHUS; cardiovascular complication; complement; extra-renal TMA; gastrointestinal complications; neurovascular complications.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources