

A structural and functional acromegaly classification
- PMID: 25250634
- PMCID: PMC4283008
- DOI: 10.1210/jc.2014-2468
A structural and functional acromegaly classification
Abstract
Context: GH-secreting pituitary adenomas exhibit heterogeneous natural history ranging from small tumors to large aggressive adenomas.
Objective: To rigorously classify an acromegaly patient cohort defined by clinical, radiological, histopathological, and outcome characteristics.
Design: Cross-sectional study.
Setting: Tertiary referral pituitary center.
Patients: Subjects were selected from a pituitary tumor research registry that includes 1178 patients with pituitary disease. Cluster analysis was performed on 338 acromegaly patients.
Interventions: None.
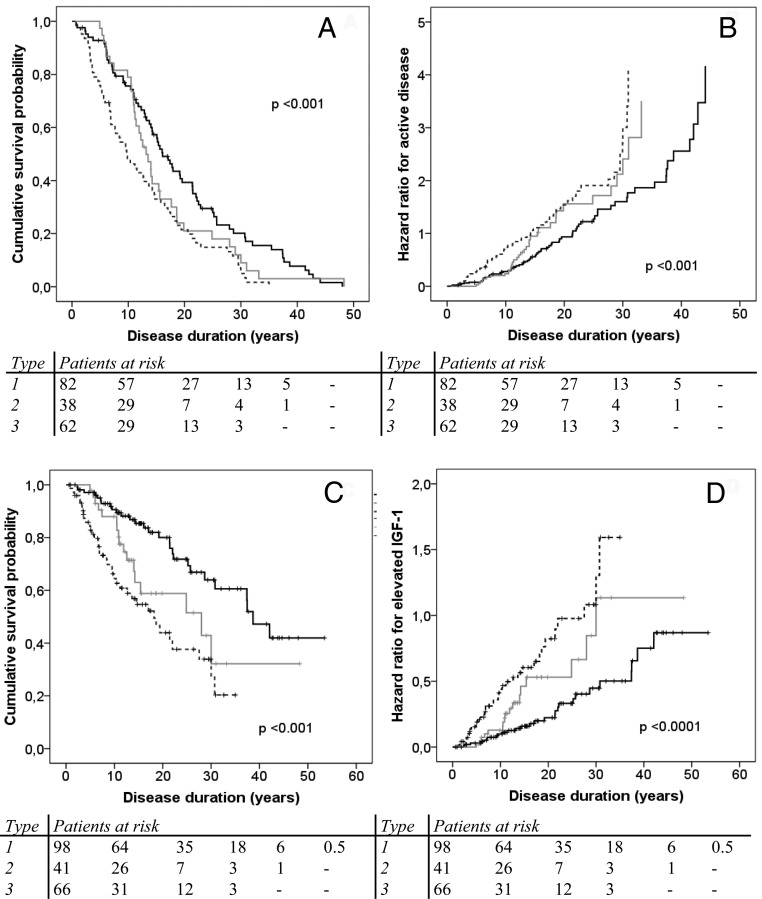
Main outcome measures: Biochemically active disease with elevated IGF-1 levels at follow-up.
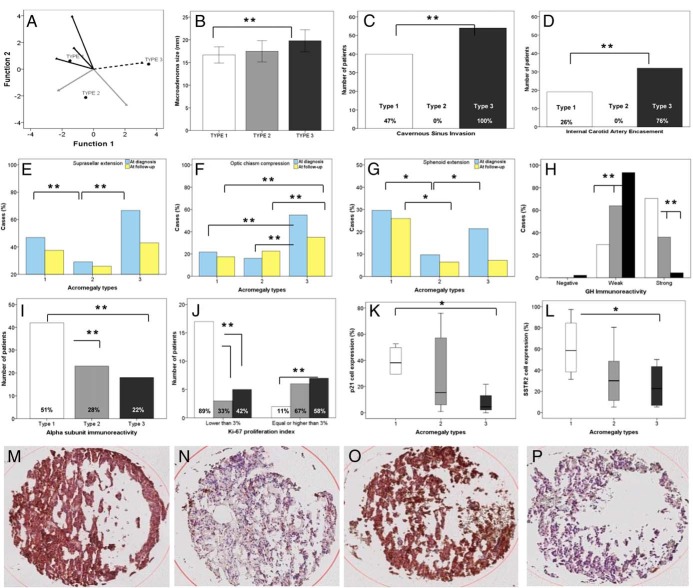
Results: Cluster analysis of all patients yielded 292 who were rigorously classified to three acromegaly types. Type 1 (50%) comprised older patients with the longest follow-up and most favorable outcomes, characterized by densely granulated, nonaggressive microadenomas and macroadenomas. Type 1 tumors extend to the sphenoid sinus more frequently than suprasellar extension (concave tumor image) and express abundant immunoreactive p21 and somatostatin receptor 2. Type 2 (19%) comprised noninvasive, densely or sparsely granulated macroadenomas, without significant extension (flat tumor image), with intermediate biochemical outcome. Type 3 (31%) was characterized by sparsely granulated aggressive macroadenomas and comprised patients with adverse therapeutic outcomes, despite receiving more treatments. These tumors extend to both the sphenoid sinus and suprasellar regions with commonly encountered optic chiasm compression ("peanut" magnetic resonance image), with low tumor p21 and somatostatin receptor 2 expression.
Conclusions: After validation, this classification may be useful to accurately identify acromegaly patients with distinctive patterns of disease aggressiveness and outcome, as well as to provide an accurate tool for selection criteria in clinical studies.
Figures
References
-
- Melmed S. Medical progress: acromegaly. N Engl J Med. 2006;355:2558–2573. - PubMed
-
- Annamalai AK, Webb A, Kandasamy N, et al. A comprehensive study of clinical, biochemical, radiological, vascular, cardiac, and sleep parameters in an unselected cohort of patients with acromegaly undergoing presurgical somatostatin receptor ligand therapy. J Clin Endocrinol Metab. 2013;98:1040–1050. - PubMed
-
- Jane JA, Jr, Starke RM, Elzoghby MA, et al. Endoscopic transsphenoidal surgery for acromegaly: remission using modern criteria, complications, and predictors of outcome. J Clin Endocrinol Metab. 2011;96:2732–2740. - PubMed
-
- Melmed S, Braunstein GD, Horvath E, Ezrin C, Kovacs K. Pathophysiology of acromegaly. Endocr Rev. 1983;4:271–290. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
