

Comparison of 2 family therapies for adolescent anorexia nervosa: a randomized parallel trial
- PMID: 25250660
- PMCID: PMC6169309
- DOI: 10.1001/jamapsychiatry.2014.1025
Comparison of 2 family therapies for adolescent anorexia nervosa: a randomized parallel trial
Abstract
Importance: Anorexia nervosa (AN) is a serious disorder with high rates of morbidity and mortality. Family-based treatment (FBT) is an evidence-based therapy for adolescent AN, but less than half of those who receive this approach recover. Hence, it is important to identify other approaches to prevent the development of the chronic form of AN for which there is no known evidence-based treatment.
Objective: To compare FBT with systemic family therapy (SyFT) for the treatment of adolescent-onset AN.
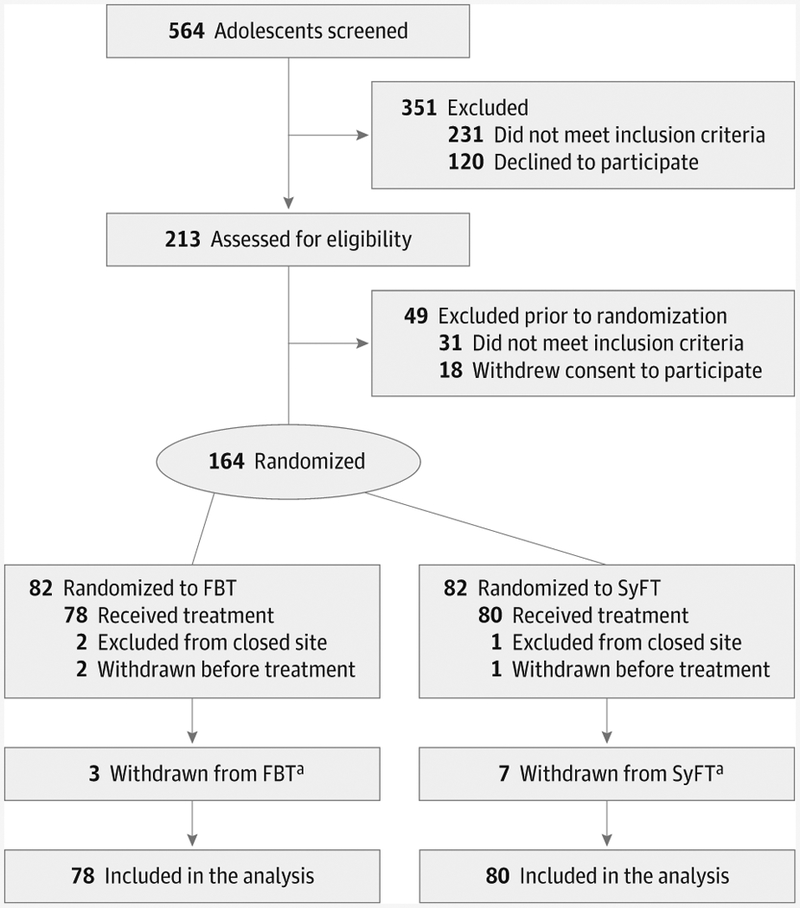
Design, setting, and participants: Research in Anorexia Nervosa (RIAN) is a 2-group (FBT and SyFT) randomized trial conducted between September 2005 and April 2012. Interviewers were blinded to the treatment condition. A total of 564 adolescents receiving care at 6 outpatient clinics experienced in the treatment of AN were screened. Of these, 262 adolescents did not meet the inclusion criteria and 138 declined to participate; hence, 164 adolescents (aged 12-18 years) of both sexes meeting the criteria for Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, AN (except for amenorrhea) were enrolled. Three participants were withdrawn from FBT and 7 were withdrawn from SyFT after serious adverse events occurred.
Interventions: Two manualized family therapies with 16 one-hour sessions during 9 months. Family-based therapy focuses on the facilitation of weight gain, whereas SyFT addresses general family processes.
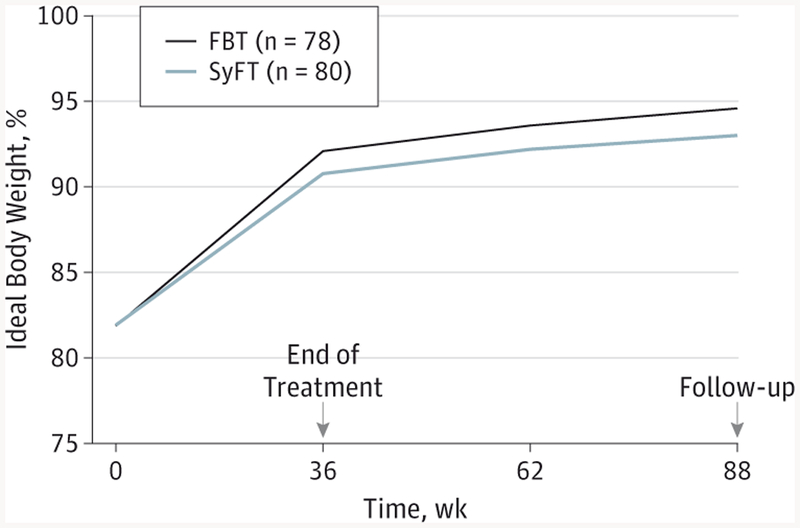
Main outcomes and measures: The primary outcomes were percentage of ideal body weight (IBW) and remission (≥95% of IBW). The a priori hypothesis was that FBT would result in faster weight gain early in treatment and at the end of treatment (EOT).
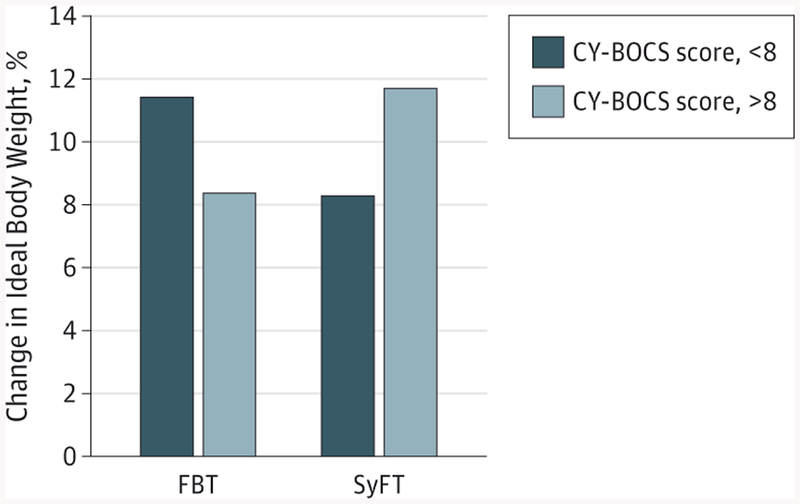
Results: There were no statistically significant differences between treatment groups for the primary outcome, for eating disorder symptoms or comorbid psychiatric disorders at the EOT or follow-up. Remission rates included FBT, 33.1% at the EOT and 40.7% at follow-up and SyFT, 25.3% and 39.0%, respectively. Family-based therapy led to significantly faster weight gain early in treatment, significantly fewer days in the hospital, and lower treatment costs per patient in remission at the EOT (FBT, $8963; SyFT, $18 005). An exploratory moderator analysis found that SyFT led to greater weight gain than did FBT for participants with more severe obsessive-compulsive symptoms.
Conclusions and relevance: The findings of this study suggest that FBT is the preferred treatment for adolescent AN because it is not significantly different from SyFT and leads to similar outcomes at a lower cost than SyFT. Adolescents with more severe obsessive-compulsive symptoms may receive more benefits with SyFT.
Trial registration: clinicaltrials.gov Identifier NCT00610753.
Conflict of interest statement
Figures
References
-
- Bulik CM, Berkman ND, Brownley KA, Sedway JA, Lohr KN. Anorexia nervosa treatment: a systematic review of randomized controlled trials. Int J Eat Disord. 2007;40(4):310–320. - PubMed
-
- Watson HJ, Bulik CM. Update on the treatment of anorexia nervosa: review of clinical trials, practice guidelines and emerging interventions. Psychol Med 2013;43(12):2477–2500. - PubMed
-
- Harris EC, Barraclough B. Excess mortality of mental disorders. Br J Psychiatry. 1988;173:11–53. - PubMed
-
- Minuchin S, Baker L, Rosman BL, Liebman R, Milman L, Todd TC. A conceptual model of psychosomatic illness in children: family organization and family therapy. Arch Gen Psychiatry. 1975;32(8): 1031–1038. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
