

Comparison of lower extremity atherosclerosis in diabetic and non-diabetic patients using multidetector computed tomography
- PMID: 25252783
- PMCID: PMC4182836
- DOI: 10.1186/1471-2261-14-125
Comparison of lower extremity atherosclerosis in diabetic and non-diabetic patients using multidetector computed tomography
Abstract
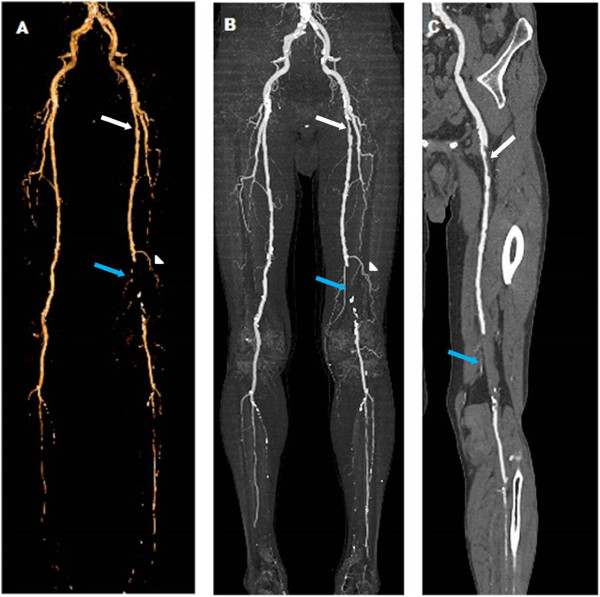
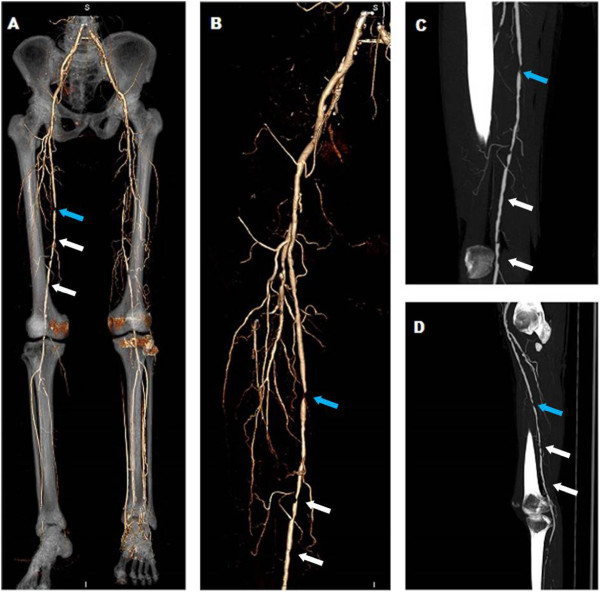
Background: Lower extremity atherosclerosis (LEA) is among the most serious diabetic complications and leads to non-traumatic amputations. The recently developed dual-source CT (DSCT) and 320- multidetector computed tomography (MDCT) may help to detect plaques more precisely. The aim of our study was to evaluate the differences in LEA between diabetic and non-diabetic patients using MDCT angiography.
Methods: DSCT and 320-MDCT angiographies of the lower extremities were performed in 161 patients (60 diabetic and 101 non-diabetic). The plaque type, distribution, shape and obstructive natures were compared.
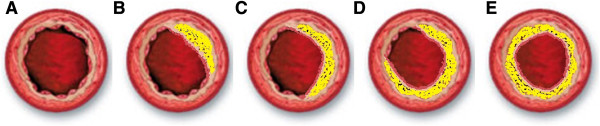
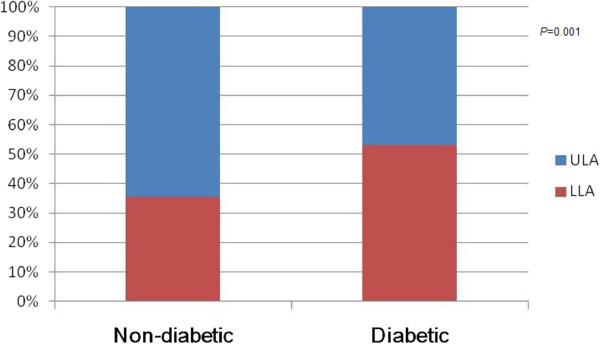
Results: Compared with non-diabetic patients, diabetic patients had higher peripheral neuropathy, history of cerebrovascular infarction and hypertension rates. A total of 2898 vascular segments were included in the analysis. Plaque and stenosis were detected in 681 segments in 60 diabetic patients (63.1%) and 854 segments in 101 non-diabetic patients (46.9%; p <0.05). Regarding these plaques, diabetic patients had a higher incidence of mixed plaques (34.2% vs. 27.1% for non-diabetic patients). An increased moderate stenosis rate and decreased occlusion rate were observed in diabetic patients relative to non-diabetic patients (35.8% vs. 28.3%; and 6.6% vs. 11.4%; respectively). In diabetic patients, 362 (53.2%) plaques were detected in the distal lower leg segments, whereas in non-diabetic patients, 551 (64.5%) plaques were found in the proximal upper leg segments. The type IV plaque shape, in which the full lumen was involved, was detected more frequently in diabetic patients than in non-diabetic patients (13.1% vs. 8.2%).
Conclusion: Diabetes is associated with a higher incidence of plaque, increased incidence of mixed plaques, moderate stenosis and localisation primarily in the distal lower leg segments. The advanced and non-invasive MDCT could be used for routine preoperative evaluations of LEA.
Figures
Similar articles
-
Application of Dual-Source CT Coronary Angiography in Type 2 Diabetic Patients with Symptomatic Coronary Heart Disease.Curr Vasc Pharmacol. 2017;15(1):59-65. doi: 10.2174/1570161114666160914175627. Curr Vasc Pharmacol. 2017. PMID: 27633455
-
Noninvasive assessment of the prevalence and characteristics of coronary atherosclerotic plaques by multidetector computed tomography in asymptomatic type 2 diabetic patients at high risk of significant coronary artery disease: a preliminary study.Arch Cardiovasc Dis. 2009 Aug-Sep;102(8-9):607-15. doi: 10.1016/j.acvd.2009.04.007. Epub 2009 Jun 25. Arch Cardiovasc Dis. 2009. PMID: 19786264
-
Usefulness of the Bollinger scoring method in evaluating peripheral artery angiography with 64-low computed tomography in patients with peripheral arterial disease.Int Angiol. 2014 Oct;33(5):426-33. Int Angiol. 2014. PMID: 25294283
-
A Review of Distribution of Atherosclerosis in the Lower Limb Arteries of Patients With Diabetes Mellitus and Peripheral Vascular Disease.Vasc Endovascular Surg. 2018 Oct;52(7):535-542. doi: 10.1177/1538574418791622. Epub 2018 Aug 1. Vasc Endovascular Surg. 2018. PMID: 30068238 Review.
-
Medial arterial calcification of the lower limbs in diabetes: Time for awareness? A short narrative review.Diabetes Metab. 2025 Jan;51(1):101586. doi: 10.1016/j.diabet.2024.101586. Epub 2024 Nov 7. Diabetes Metab. 2025. PMID: 39521119 Review.
Cited by
-
Race and Socioeconomic Status Independently Affect Risk of Major Amputation in Peripheral Artery Disease.J Am Heart Assoc. 2018 Jan 12;7(2):e007425. doi: 10.1161/JAHA.117.007425. J Am Heart Assoc. 2018. PMID: 29330260 Free PMC article.
-
Multi-Modality Imaging of Atheromatous Plaques in Peripheral Arterial Disease: Integrating Molecular and Imaging Markers.Int J Mol Sci. 2023 Jul 5;24(13):11123. doi: 10.3390/ijms241311123. Int J Mol Sci. 2023. PMID: 37446302 Free PMC article. Review.
-
Descriptive Analysis of Anatomical Location and Metabolic and Microbiological Factors in Diabetic Foot (DF) Treated at a DF Specialty Tertiary Care Hospital With a Multidisciplinary Approach.Cureus. 2025 Mar 16;17(3):e80690. doi: 10.7759/cureus.80690. eCollection 2025 Mar. Cureus. 2025. PMID: 40242699 Free PMC article.
-
[Diagnostic accuracy of dual energy CT angiography in patients with diabetes mellitus].Radiologe. 2015 Apr;55(4):314-22. doi: 10.1007/s00117-014-2721-8. Radiologe. 2015. PMID: 25809927 German.
References
-
- Scholte AJ, Schuijf JD, Kharagjitsingh AV, Jukema JW, Pundziute G, van der Wall EE, Bax JJ. Prevalence of coronary artery disease and plaque morphology assessed by multi-slice computed tomography coronary angiography and calcium scoring in asymptomatic patients with type 2 diabetes. Heart. 2008;94(3):290–295. doi: 10.1136/hrt.2007.121921. - DOI - PubMed
-
- Ohnishi H, Sawayama Y, Furusyo N, Maeda S, Tokunaga S, Hayashi J. Risk factors for and the prevalence of peripheral arterial disease and its relationship to carotid atherosclerosis: the Kyushu and Okinawa Population Study (KOPS) J Atheroscler Thromb. 2010;17(7):751–758. doi: 10.5551/jat.3731. - DOI - PubMed
-
- Nguyen LL, Hevelone N, Rogers SO, Bandyk DF, Clowes AW, Moneta GL, Lipsitz S, Conte MS. Disparity in outcomes of surgical revascularization for limb salvage: race and gender are synergistic determinants of vein graft failure and limb loss. Circulation. 2009;119(1):123–130. doi: 10.1161/CIRCULATIONAHA.108.810341. - DOI - PMC - PubMed
Pre-publication history
-
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2261/14/125/prepub
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
