

Inter- and intralaboratory comparison of JC polyomavirus antibody testing using two different virus-like particle-based assays
- PMID: 25253664
- PMCID: PMC4248761
- DOI: 10.1128/CVI.00489-14
Inter- and intralaboratory comparison of JC polyomavirus antibody testing using two different virus-like particle-based assays
Abstract
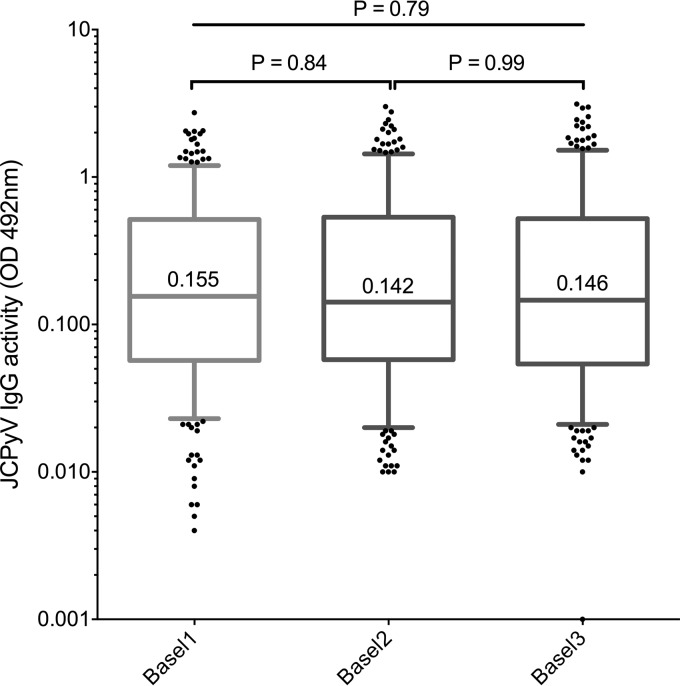
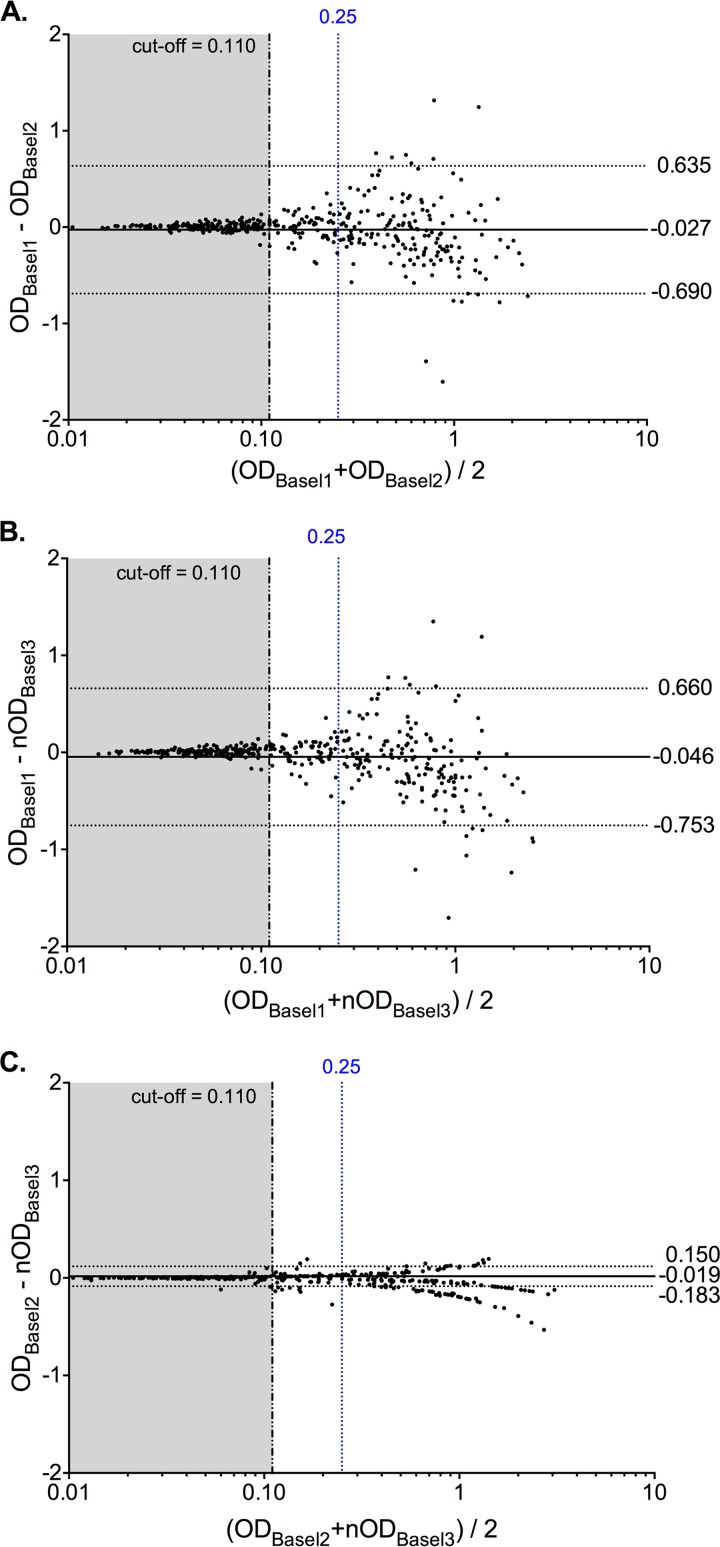
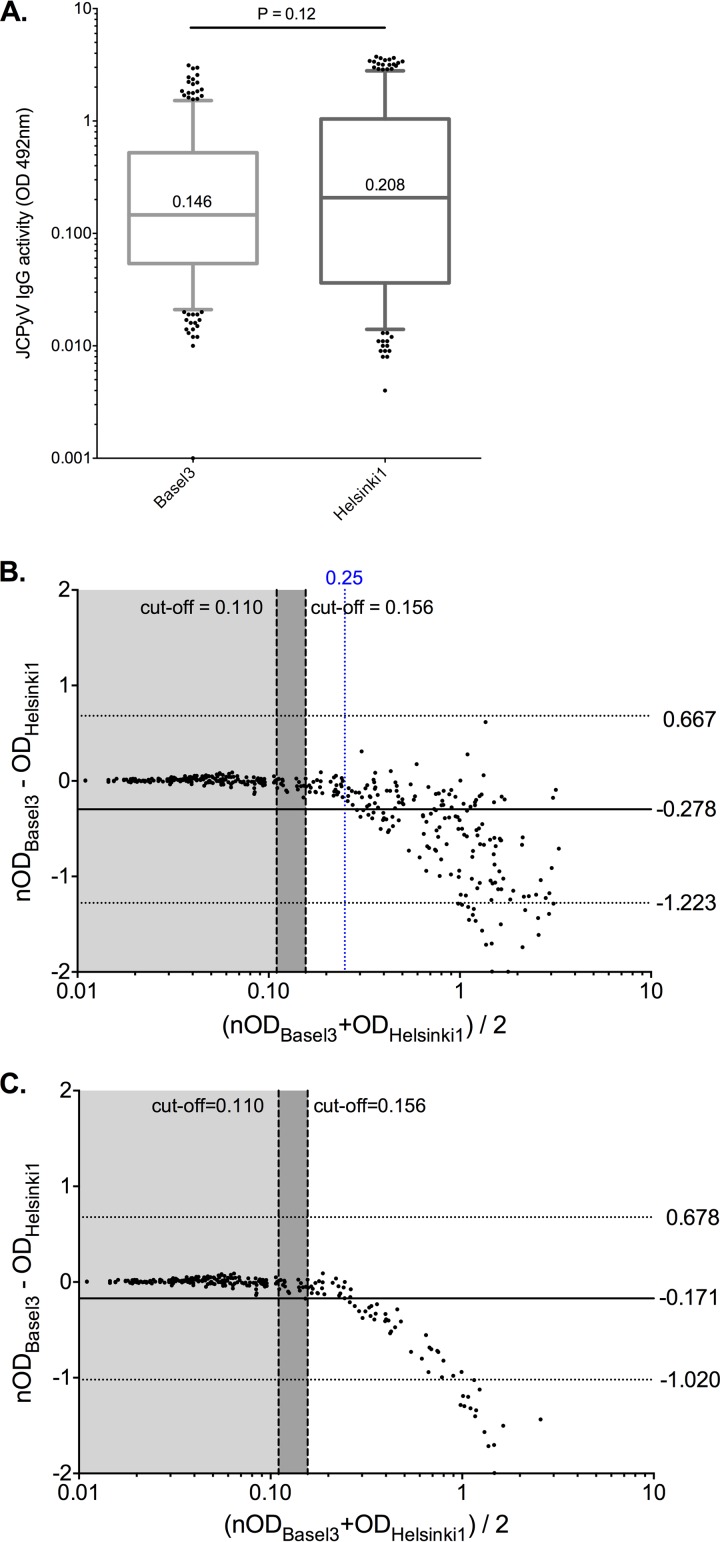
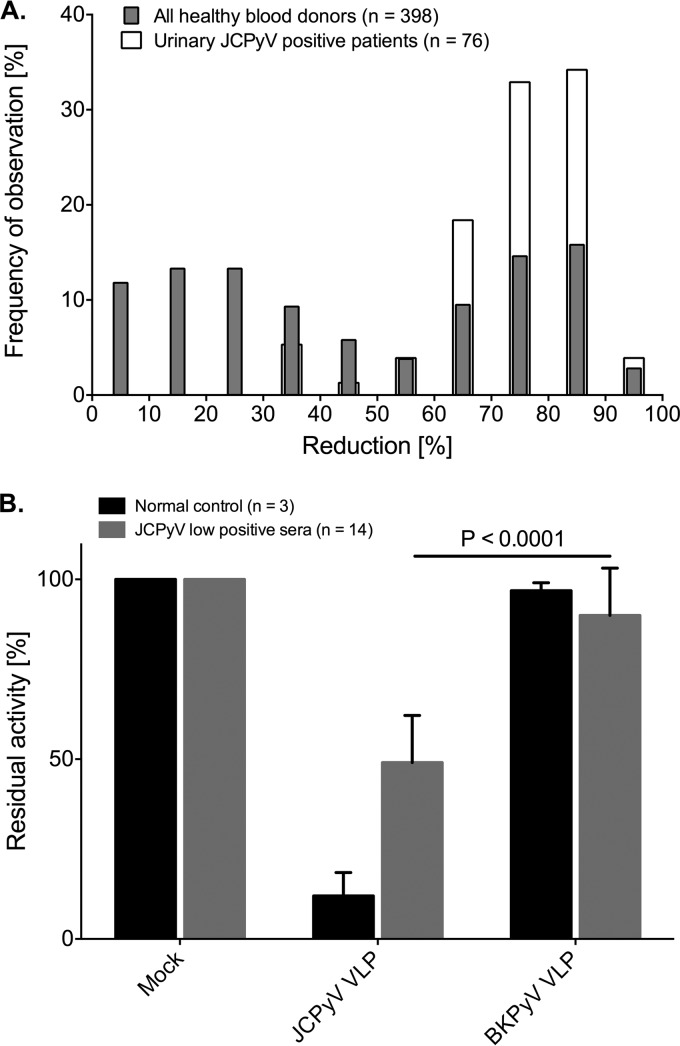
JC polyomavirus (JCPyV) can cause progressive multifocal leukoencephalopathy (PML), a debilitating, often fatal brain disease in immunocompromised patients. JCPyV-seropositive multiple sclerosis (MS) patients treated with natalizumab have a 2- to 10-fold increased risk of developing PML. Therefore, JCPyV serology has been recommended for PML risk stratification. However, different antibody tests may not be equivalent. To study intra- and interlaboratory variability, sera from 398 healthy blood donors were compared in 4 independent enzyme-linked immunoassay (ELISA) measurements generating >1,592 data points. Three data sets (Basel1, Basel2, and Basel3) used the same basic protocol but different JCPyV virus-like particle (VLP) preparations and introduced normalization to a reference serum. The data sets were also compared with an independent method using biotinylated VLPs (Helsinki1). VLP preadsorption reducing ≥35% activity was used to identify seropositive sera. The results indicated that Basel1, Basel2, Basel3, and Helsinki1 were similar regarding overall data distribution (P = 0.79) and seroprevalence (58.0, 54.5, 54.8, and 53.5%, respectively; P = 0.95). However, intra-assay intralaboratory comparison yielded 3.7% to 12% discordant results, most of which were close to the cutoff (0.080 < optical density [OD] < 0.250) according to Bland-Altman analysis. Introduction of normalization improved overall performance and reduced discordance. The interlaboratory interassay comparison between Basel3 and Helsinki1 revealed only 15 discordant results, 14 (93%) of which were close to the cutoff. Preadsorption identified specificities of 99.44% and 97.78% and sensitivities of 99.54% and 95.87% for Basel3 and Helsinki1, respectively. Thus, normalization to a preferably WHO-approved reference serum, duplicate testing, and preadsorption for samples around the cutoff may be necessary for reliable JCPyV serology and PML risk stratification.
Copyright © 2014, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Ferenczy MW, Marshall LJ, Nelson CD, Atwood WJ, Nath A, Khalili K, Major EO. 2012. Molecular biology, epidemiology, and pathogenesis of progressive multifocal leukoencephalopathy, the JC virus-induced demyelinating disease of the human brain. Clin. Microbiol. Rev. 25:471–506. 10.1128/CMR.05031-11. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
