

Successful surgical strategy in a late case of Boerhaave's syndrome
- PMID: 25253979
- PMCID: PMC4168112
- DOI: 10.3748/wjg.v20.i35.12696
Successful surgical strategy in a late case of Boerhaave's syndrome
Abstract
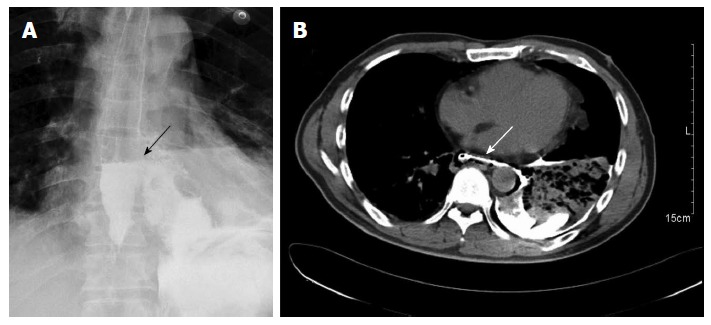
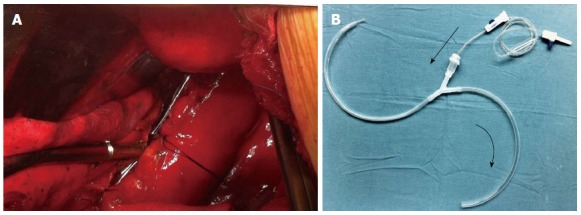
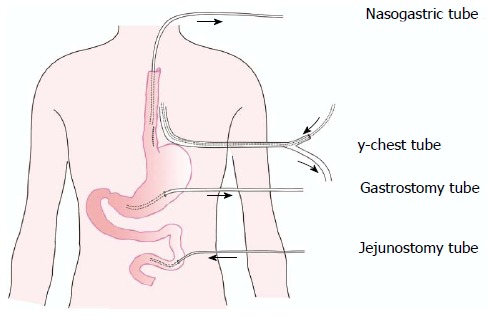
Boerhaave's syndrome refers to the spontaneous transmural rupture of the esophagus. Primary repair may be performed in patients who present within 24 h of perforation, and such cases have the best outcomes as most complications have not yet developed. However, the treatment of late perforations remains controversial. Various approaches and strategies to repair late perforations have been described in the literature, but there is no uniform approach. We present a case of Boerhaave's syndrome in which the patient underwent surgical repair 48 h after the acute event and was subsequently treated successfully. The initial approach included direct esophageal repair, a drainage series, and nutritional support via a feeding jejunostomy. Although the repair site was subsequently disrupted, the patient showed complete healing of the perforation after three weeks. We consider that our surgical treatment strategy is safe and technically feasible, and appears to be a promising alternative approach for the treatment of patients with late Boerhaave's perforation.
Keywords: Boerhaave’s perforation; Drainage; Nutritional support; Repair; Surgery.
Figures

References
-
- Richardson JD. Management of esophageal perforations: the value of aggressive surgical treatment. Am J Surg. 2005;190:161–165. - PubMed
-
- Chirica M, Champault A, Dray X, Sulpice L, Munoz-Bongrand N, Sarfati E, Cattan P. Esophageal perforations. J Visc Surg. 2010;147:e117–e128. - PubMed
-
- Khan AZ, Strauss D, Mason RC. Boerhaave’s syndrome: diagnosis and surgical management. Surgeon. 2007;5:39–44. - PubMed
-
- Wolfson D, Barkin JS. Treatment of Boerhaave’s Syndrome. Curr Treat Options Gastroenterol. 2007;10:71–77. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
