

Giant cell arteritis: a systematic review of the qualitative and semiquantitative methods to assess vasculitis with 18F-fluorodeoxyglucose positron emission tomography
- PMID: 25254211
- PMCID: PMC4165737
- DOI: 10.1155/2014/574248
Giant cell arteritis: a systematic review of the qualitative and semiquantitative methods to assess vasculitis with 18F-fluorodeoxyglucose positron emission tomography
Abstract
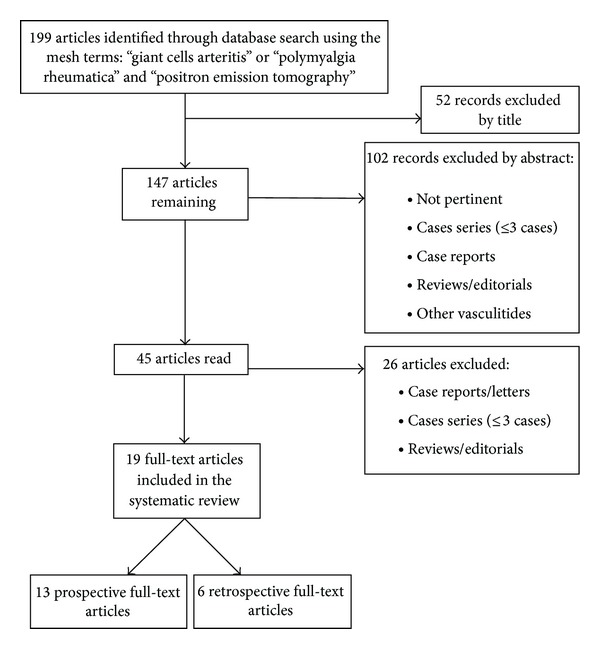
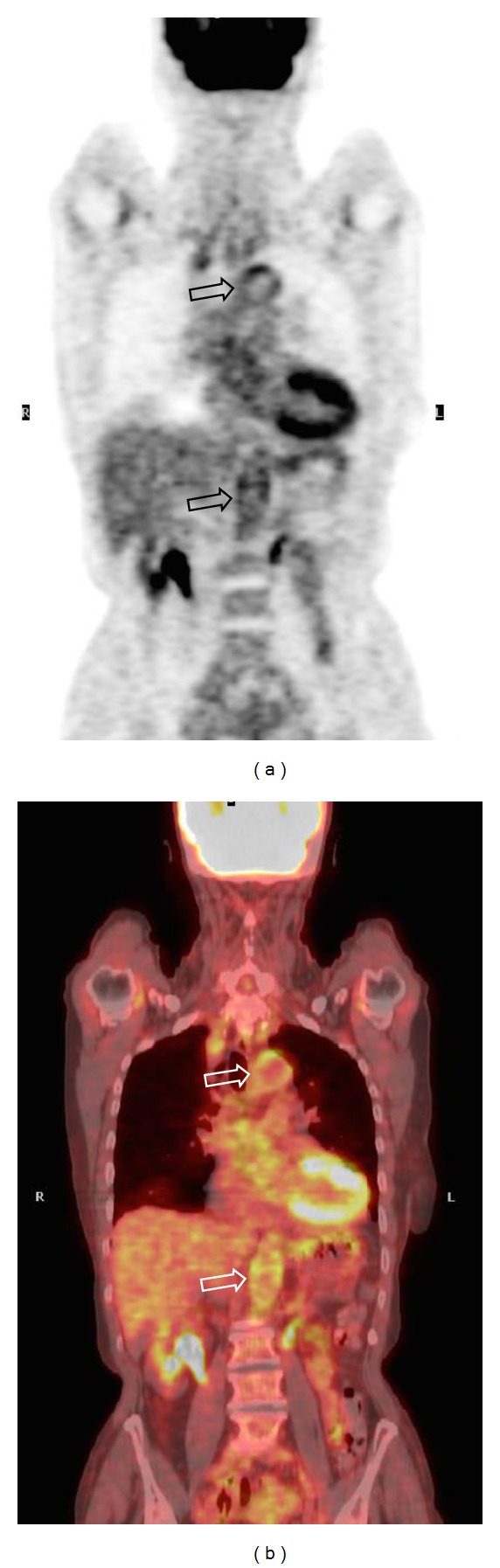
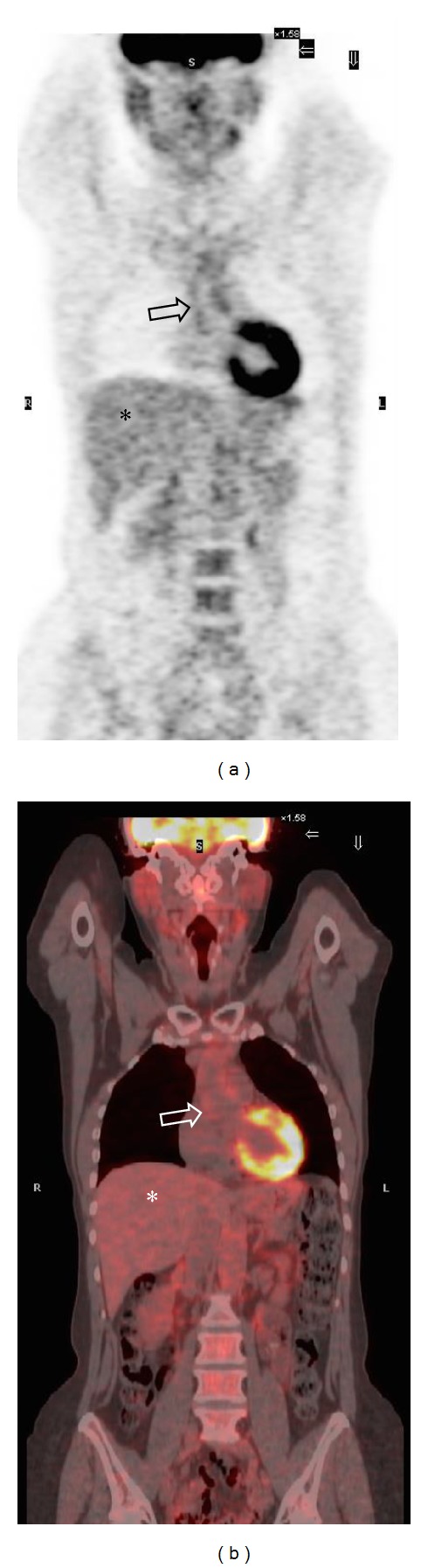
Giant cell arteritis (GCA) is the most common vasculitis affecting medium and large vessels. It shows a close clinical association with polymyalgia rheumatica (PMR), a musculoskeletal inflammatory disorder, which is clinically characterized by girdles pain and stiffness. 18F-Fluorodeoxyglucose (18F-FDG) positron emission tomography (PET) is an effective tool for the diagnosis, grading, and follow-up of patients affected by GCA involving the aorta and its proximal branches, but the lack of a standardized method for the assessment of vascular inflammation remains a critical issue, potentially leading to misclassification. In our systematic review, including 19 original articles for a total of 442 GCA patients (with or without PMR symptoms) and 535 healthy controls, we described the different qualitative, semiquantitative and combined methods that have been proposed throughout the literature for assessing the presence and grading the severity of GCA-related vascular inflammation on 18F-FDG PET scans, focusing on the diagnostic performance and examining their respective advantages and limitations. The majority of the included studies adopted qualitative methods of PET image analysis, which are less sensitive but more specific than semiquantitative ones. Among the semiquantitative approaches, the aortic-to-blood pool uptake ratio of the aortic arch seems to be the most accurate method.
Figures


Similar articles
-
Low incidence of late-onset giant cell arteritis during the first year in patients with polymyalgia rheumatica-a repeated imaging study.Rheumatology (Oxford). 2025 Apr 1;64(4):2193-2198. doi: 10.1093/rheumatology/keae463. Rheumatology (Oxford). 2025. PMID: 39180419
-
Management of large-vessel vasculitis with FDG-PET: a systematic literature review and meta-analysis.Medicine (Baltimore). 2015 Apr;94(14):e622. doi: 10.1097/MD.0000000000000622. Medicine (Baltimore). 2015. PMID: 25860208 Free PMC article.
-
Polymyalgia Rheumatica and Giant Cell Arteritis: A Systematic Review.JAMA. 2016 Jun 14;315(22):2442-58. doi: 10.1001/jama.2016.5444. JAMA. 2016. PMID: 27299619
-
Positron emission tomography-adapted therapy for first-line treatment in individuals with Hodgkin lymphoma.Cochrane Database Syst Rev. 2015 Jan 9;1(1):CD010533. doi: 10.1002/14651858.CD010533.pub2. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2025 Mar 26;3:CD010533. doi: 10.1002/14651858.CD010533.pub3. PMID: 25572491 Free PMC article. Updated.
-
123I-MIBG scintigraphy and 18F-FDG-PET imaging for diagnosing neuroblastoma.Cochrane Database Syst Rev. 2015 Sep 29;2015(9):CD009263. doi: 10.1002/14651858.CD009263.pub2. Cochrane Database Syst Rev. 2015. PMID: 26417712 Free PMC article.
Cited by
-
18F-fluorodeoxyglucose positron emission tomography and the risk of subsequent aortic complications in giant-cell arteritis: A multicenter cohort of 130 patients.Medicine (Baltimore). 2016 Jun;95(26):e3851. doi: 10.1097/MD.0000000000003851. Medicine (Baltimore). 2016. PMID: 27367985 Free PMC article.
-
Giant-cell arteritis without cranial manifestations: Working diagnosis of a distinct disease pattern.Medicine (Baltimore). 2016 Jun;95(26):e3818. doi: 10.1097/MD.0000000000003818. Medicine (Baltimore). 2016. PMID: 27367984 Free PMC article.
-
Semi-Quantitative and Quantitative [18F]FDG-PET/CT Indices for Diagnosing Large Vessel Vasculitis: A Critical Review.Diagnostics (Basel). 2021 Dec 14;11(12):2355. doi: 10.3390/diagnostics11122355. Diagnostics (Basel). 2021. PMID: 34943593 Free PMC article. Review.
-
The value of ultrasound in diagnosing extracranial large-vessel vasculitis compared to FDG-PET/CT: A retrospective study.Clin Rheumatol. 2017 Sep;36(9):2079-2086. doi: 10.1007/s10067-017-3669-7. Epub 2017 May 15. Clin Rheumatol. 2017. PMID: 28503707
-
F-18 FDG PET for assessment of disease activity of large vessel vasculitis: A systematic review and meta-analysis.J Nucl Cardiol. 2019 Feb;26(1):59-67. doi: 10.1007/s12350-018-1406-5. Epub 2018 Aug 17. J Nucl Cardiol. 2019. PMID: 30120746
References
-
- Salvarani C, Cantini F, Boiardi L, Hunder GG. Polymyalgia rheumatica and giant-cell arteritis. New England Journal of Medicine. 2002;347(4):261–271. - PubMed
-
- Gonzalez-Gay MA, Garcia-Porrua C, Miranda-Filloy JA, Martin J. Giant cell arteritis and polymyalgia rheumatica: pathophysiology and management. Drugs and Aging. 2006;23(8):627–649. - PubMed
-
- Nuenninghoff DM, Hunder GG, Christianson TJH, McClelland RL, Matteson EL. Incidence and predictors of large-artery complication (aortic aneurysm, aortic dissection, and/or large-artery stenosis) in patients with giant cell arteritis: a population-based study over 50 years. Arthritis and Rheumatism. 2003;48(12):3522–3531. - PubMed
-
- Evans JM, O'Fallon WM, Hunder GG. Increased incidence of aortic aneurysm and dissection in giant cell (temporal) arteritis: a population-based study. Annals of Internal Medicine. 1995;122(7):502–507. - PubMed
-
- Bongartz T, Matteson EL. Large-vessel involvement in giant cell arteritis. Current Opinion in Rheumatology. 2006;18(1):10–17. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
