

Do intravenous N-acetylcysteine and sodium bicarbonate prevent high osmolal contrast-induced acute kidney injury? A randomized controlled trial
- PMID: 25254489
- PMCID: PMC4177831
- DOI: 10.1371/journal.pone.0107602
Do intravenous N-acetylcysteine and sodium bicarbonate prevent high osmolal contrast-induced acute kidney injury? A randomized controlled trial
Abstract
Background: N-acetylcysteine (NAC) or sodium bicarbonate (NaHCO3), singly or combined, inconsistently prevent patients exposed to radiographic contrast media from developing contrast-induced acute kidney injury (CI-AKI).
Objective: We asked whether intravenous isotonic saline and either NaHCO3 in 5% dextrose or else a high dose of NAC in 5% dextrose prevent CI-AKI in outpatients exposed to high-osmolal iodinated contrast medium more than does saline alone.
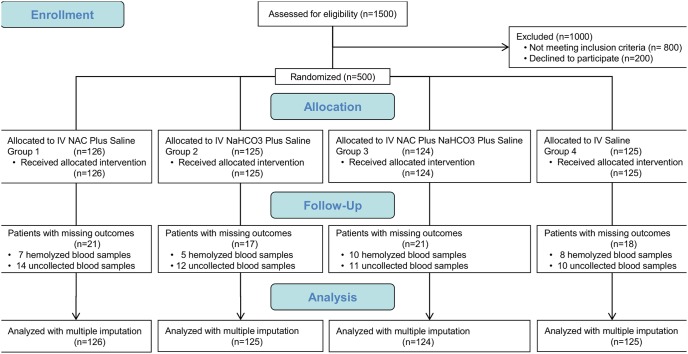
Methods: This completed prospective, parallel, superiority, open-label, controlled, computer-randomized, single-center, Brazilian trial (NCT01612013) hydrated 500 adult outpatients (214 at high risk of developing CI-AKI) exposed to ioxitalamate during elective coronary angiography and ventriculography. From 1 hour before through 6 hours after exposure, 126 patients (group 1) received a high dose of NAC and saline, 125 (group 2) received NaHCO3 and saline, 124 (group 3) received both treatments, and 125 (group 4) received only saline.
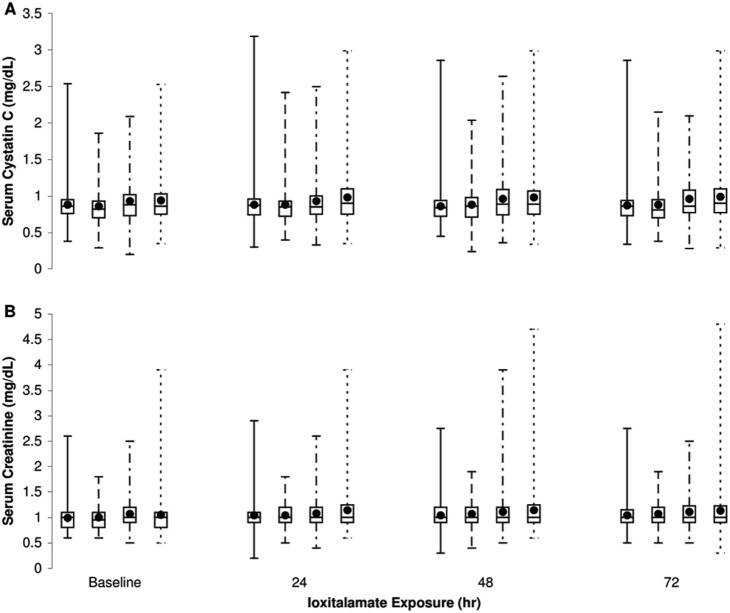
Results: Groups were similar with respect to age, gender, weight, pre-existing renal dysfunction, hypertension, medication, and baseline serum creatinine and serum cystatin C, but diabetes mellitus was significantly less prevalent in group 1. CI-AKI incidence 72 hours after exposure to contrast medium was 51.4% (257/500), measured as serum creatinine > (baseline+0.3 mg/dL) and/or serum cystatin C > (1.1 · baseline), and 7.6% (38/500), measured as both serum creatinine and serum cystatin C > (baseline+0.3 mg/dL) or > (1.25 · baseline). CI-AKI incidence measured less sensitively was similar among groups. Measured more sensitively, incidence in group 1 was significantly (p<0.05) lower than in groups 2 and 3 but not group 4; adjustment for confounding by infused volume equalized incidence in groups 1 and 3.
Conclusion: We found no evidence that intravenous isotonic saline and either NaHCO3 or else a high dose of NAC prevent CI-AKI in outpatients exposed to high osmolal iodinated contrast medium more than does saline alone.
Trial registration: ClinicalTrials.gov NCT01612013.
Conflict of interest statement
Figures
References
-
- MacCullough PA (2008) Contrast-induced acute kidney injury. J Am Coll Cardiol 51(15): 1419–1428. - PubMed
-
- Parfrey PS, Griffiths SM, Barrett BJ, Paul MD, Genge M, et al. (1989) Contrast material-induced renal failure in patients with diabetes mellitus, renal insufficiency, or both. A prospective controlled study. N Engl J Med 320(3): 143–149. - PubMed
-
- Stevens MA, McCullough PA, Tobin KJ, Speck JP, Westveer DC, et al. (1999) A prospective randomized trial of prevention measures in patients at high risk for contrast nephropathy: results of the P.R.I.N.C.E. study. Prevention of radiocontrast induced nephropathy clinical evaluation. J Am Coll Cardiol 33(2): 403–411. - PubMed
-
- Solomon R, Werner C, Mann D, D’Elia J, Silva P (1994) Effects of saline, mannitol, and furosemide to prevent acute decreases in renal function induced by radiocontrast agents. N Engl J Med 331: 1416–1420. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
