

Effects of screening and systemic adjuvant therapy on ER-specific US breast cancer mortality
- PMID: 25255803
- PMCID: PMC4271026
- DOI: 10.1093/jnci/dju289
Effects of screening and systemic adjuvant therapy on ER-specific US breast cancer mortality
Abstract
Background: Molecular characterization of breast cancer allows subtype-directed interventions. Estrogen receptor (ER) is the longest-established molecular marker.
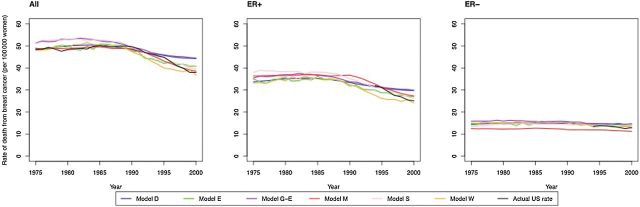
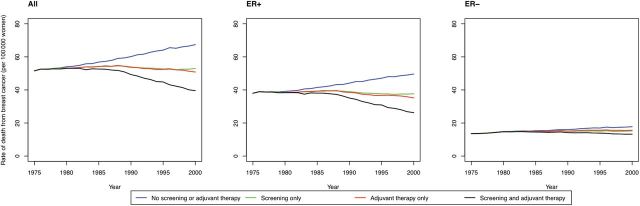
Methods: We used six established population models with ER-specific input parameters on age-specific incidence, disease natural history, mammography characteristics, and treatment effects to quantify the impact of screening and adjuvant therapy on age-adjusted US breast cancer mortality by ER status from 1975 to 2000. Outcomes included stage-shifts and absolute and relative reductions in mortality; sensitivity analyses evaluated the impact of varying screening frequency or accuracy.
Results: In the year 2000, actual screening and adjuvant treatment reduced breast cancer mortality by a median of 17 per 100000 women (model range = 13-21) and 5 per 100000 women (model range = 3-6) for ER-positive and ER-negative cases, respectively, relative to no screening and no adjuvant treatment. For ER-positive cases, adjuvant treatment made a higher relative contribution to breast cancer mortality reduction than screening, whereas for ER-negative cases the relative contributions were similar for screening and adjuvant treatment. ER-negative cases were less likely to be screen-detected than ER-positive cases (35.1% vs 51.2%), but when screen-detected yielded a greater survival gain (five-year breast cancer survival = 35.6% vs 30.7%). Screening biennially would have captured a lower proportion of mortality reduction than annual screening for ER-negative vs ER-positive cases (model range = 80.2%-87.8% vs 85.7%-96.5%).
Conclusion: As advances in risk assessment facilitate identification of women with increased risk of ER-negative breast cancer, additional mortality reductions could be realized through more frequent targeted screening, provided these benefits are balanced against screening harms.
© The Author 2014. Published by Oxford University Press. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Kurian AW, Carlson RW. Chapter 17: Principles of Breast Cancer Therapy. In: Li CI, (ed). Breast Cancer Epidemiology: Springer; 2010:371–388.
-
- Sedjo RL, Byers T, Barrera E, Jr, et al. A midpoint assessment of the American Cancer Society challenge goal to decrease cancer incidence by 25% between 1992 and 2015. CA Cancer J Clin. 2007;57(6):326–340. - PubMed
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63(1):11–30. - PubMed
-
- Esserman L, Shieh Y, Thompson I. Rethinking screening for breast cancer and prostate cancer. JAMA. 2009;302(15):1685–1692. - PubMed
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2009. CA Cancer J Clin. 2009;59(4):225–249. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
