

Differentiation between chalazion and sebaceous carcinoma by noninvasive meibography
- PMID: 25258508
- PMCID: PMC4172083
- DOI: 10.2147/OPTH.S69804
Differentiation between chalazion and sebaceous carcinoma by noninvasive meibography
Abstract
Background: Sebaceous carcinoma is notorious for masquerading clinically as other benign lesions such as chalazion. A tool to better differentiate between these two conditions would thus be desirable.
Purpose: To examine the potential application of noninvasive meibography in the differential diagnosis of chalazion and sebaceous carcinoma of the eyelid as a retrospective cross-sectional study.
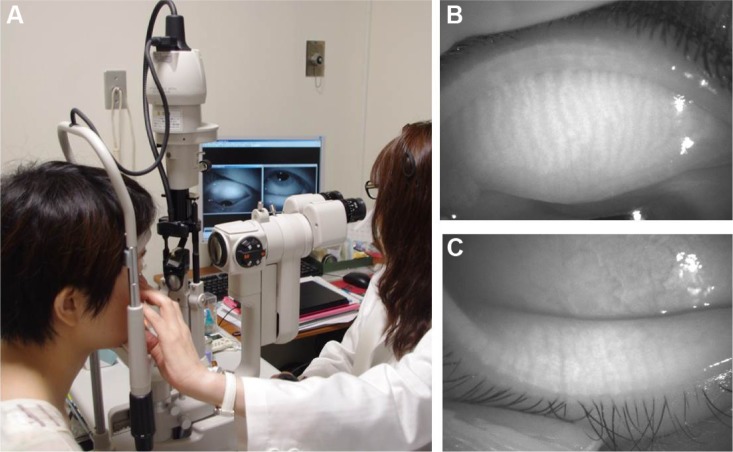
Methods: Five individuals with chalazion and three patients with sebaceous carcinoma were observed. Noninvasive meibography was performed to visualize the reflectivity and shape of the lesion in each subject.
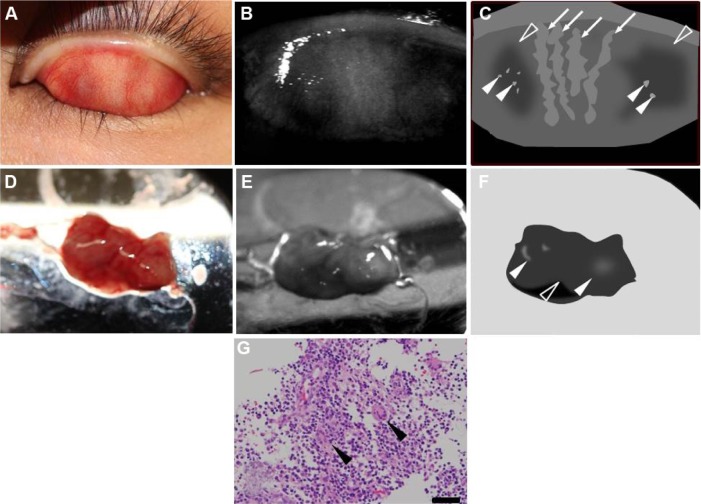
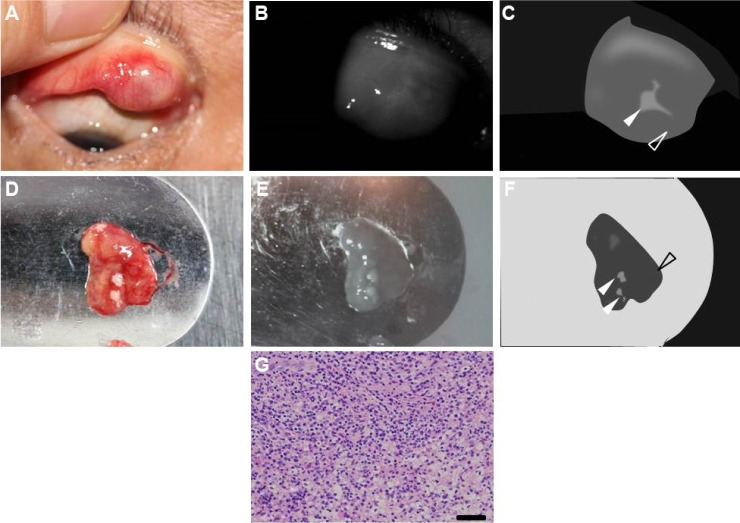
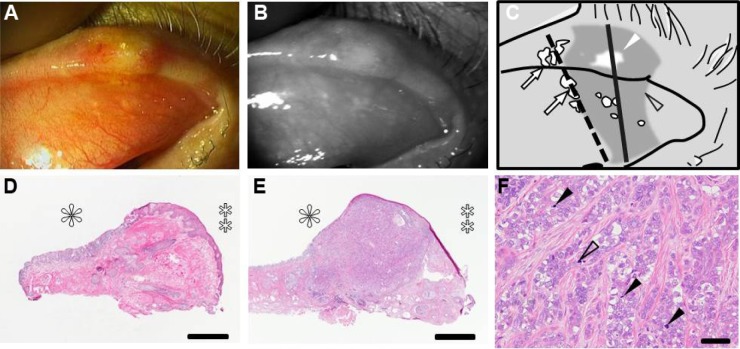
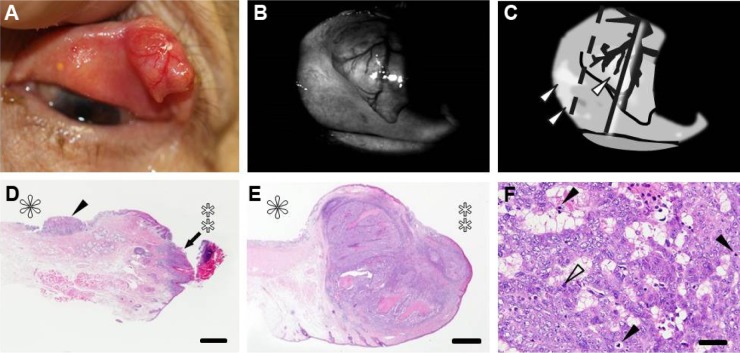
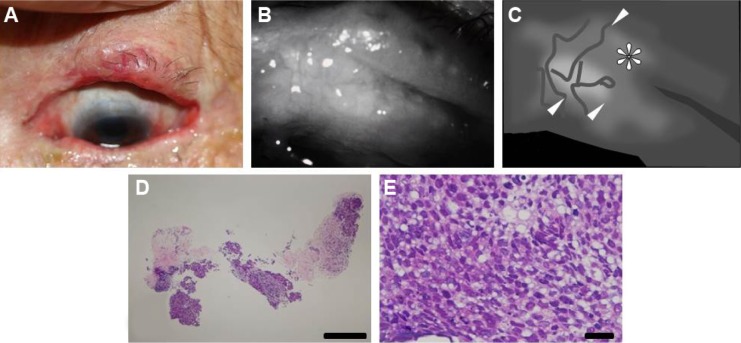
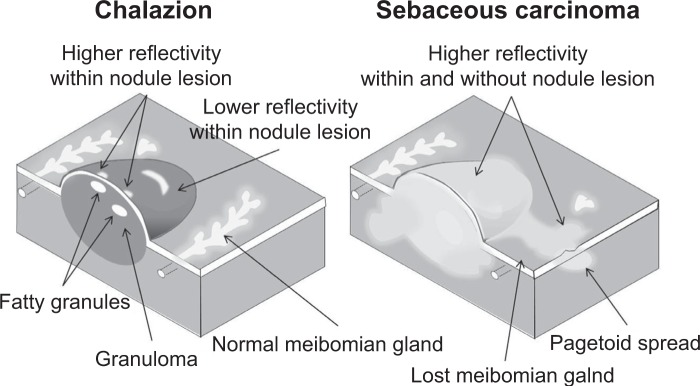
Results: Noninvasive meibographic imaging revealed chalazion as a lesion of overall low reflectivity with small regions of higher reflectivity corresponding to lipid granules. On the other hand, the noninvasive meibography revealed sebaceous carcinoma as a poorly marginated lesion of high reflectivity in the eyelid.
Conclusion: Noninvasive meibographic imaging may prove useful for the differential diagnosis of chalazion and sebaceous carcinoma. It may also be informative in definition of the resection area in carcinoma patients.
Keywords: chalazion; eyelid; noninvasive meibography; sebaceous carcinoma.
Figures
References
-
- Shields JA, Shields CL. Eyelid, Conjunctival, and Orbital Tumors. An Atlas and Textbook. 2nd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2007.
-
- Shields JA, Demirci H, Marr BP, Eagle RC, Jr, Shields CL. Sebaceous carcinoma of the eyelids: personal experience with 60 cases. Ophthalmology. 2004;111(12):2151–2157. - PubMed
-
- Keskinaslan I, Pedroli GL, Piffaretti JM, Meyer P, Kunz C, Haefliger IO. Eyelid sebaceous gland carcinoma in a young Caucasian man. Klin Monbl Augenheilkd. 2008;225(5):422–423. - PubMed
-
- Ozdal PC, Codere F, Callejo S, Caissie AL, Burnier MN. Accuracy of the clinical diagnosis of chalazion. Eye (Lond) 2004;18(2):135–138. - PubMed
-
- Arita R, Itoh K, Inoue K, Amano S. Noncontact infrared meibography to document age-related changes of the meibomian glands in a normal population. Ophthalmology. 2008;115(5):911–915. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
