

Glucose, insulin, and oxygen interplay in placental hypervascularisation in diabetes mellitus
- PMID: 25258707
- PMCID: PMC4167234
- DOI: 10.1155/2014/145846
Glucose, insulin, and oxygen interplay in placental hypervascularisation in diabetes mellitus
Abstract
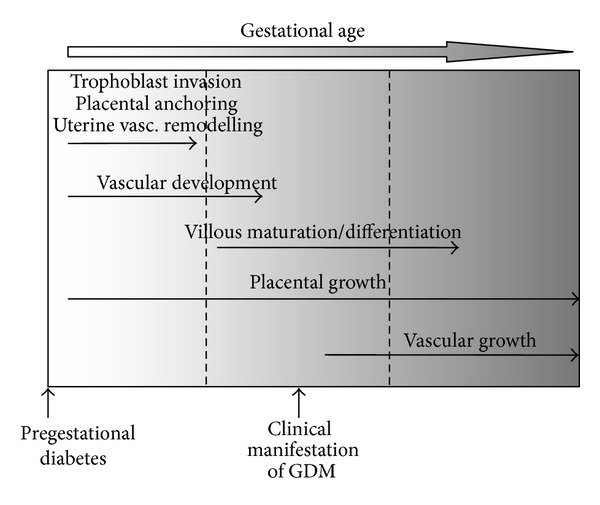
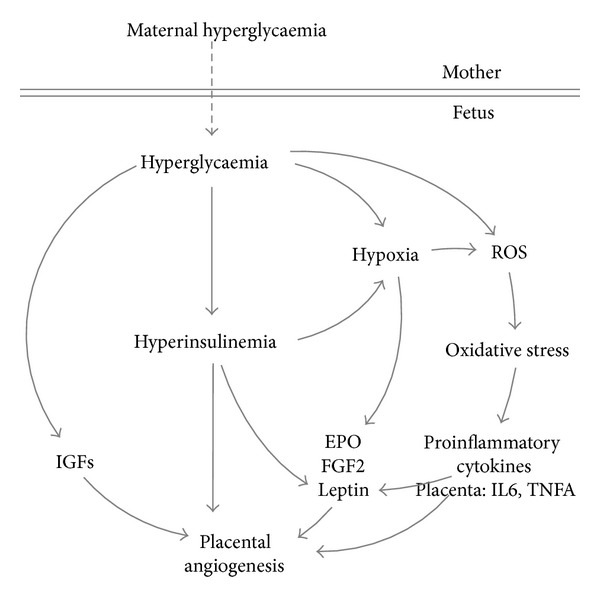
The placental vasculature rapidly expands during the course of pregnancy in order to sustain the growing needs of the fetus. Angiogenesis and vascular growth are stimulated and regulated by a variety of growth factors expressed in the placenta or present in the fetal circulation. Like in tumors, hypoxia is a major regulator of angiogenesis because of its ability to stimulate expression of various proangiogenic factors. Chronic fetal hypoxia is often found in pregnancies complicated by maternal diabetes as a result of fetal hyperglycaemia and hyperinsulinemia. Both are associated with altered levels of hormones, growth factors, and proinflammatory cytokines, which may act in a proangiogenic manner and, hence, affect placental angiogenesis and vascular development. Indeed, the placenta in diabetes is characterized by hypervascularisation, demonstrating high placental plasticity in response to diabetic metabolic derangements. This review describes the major regulators of placental angiogenesis and how the diabetic environment in utero alters their expression. In the light of hypervascularized diabetic placenta, the focus was placed on proangiogenic factors.
Figures
References
-
- Jauniaux E, Burton GJ. Villous histomorphometry and placental bed biopsy investigation in type I diabetic pregnancies. Placenta. 2006;27(4-5):468–474. - PubMed
-
- Mayhew TM. Enhanced fetoplacental angiogenesis in pre-gestational diabetes mellitus: the extra growth is exclusively longitudinal and not accompanied by microvascular remodelling. Diabetologia. 2002;45(10):1434–1439. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
