

Modeled PFOA exposure and coronary artery disease, hypertension, and high cholesterol in community and worker cohorts
- PMID: 25260175
- PMCID: PMC4256699
- DOI: 10.1289/ehp.1307943
Modeled PFOA exposure and coronary artery disease, hypertension, and high cholesterol in community and worker cohorts
Abstract
Background: Several previous studies, mostly cross-sectional, have found associations between perfluorooctanoic acid (PFOA) and high cholesterol levels, but studies of hypertension and heart disease have had inconsistent findings.
Objectives: In this study we examined the association between modeled PFOA exposure and incident hypertension, hypercholesterolemia, and coronary artery disease among workers at a Mid-Ohio Valley chemical plant that used PFOA, and residents of the surrounding community.
Methods: Community- and worker-cohort participants completed surveys during 2008-2011 covering demographics, health-related behaviors, and medical history. Cox proportional hazard models, stratified by birth year, modeled the hazard of each outcome (starting at 20 years of age) as a function of retrospective serum PFOA concentration estimates (generated through fate, transport and exposure modeling), controlling for sex, race, education, smoking, alcohol use, body mass index, and diabetes.
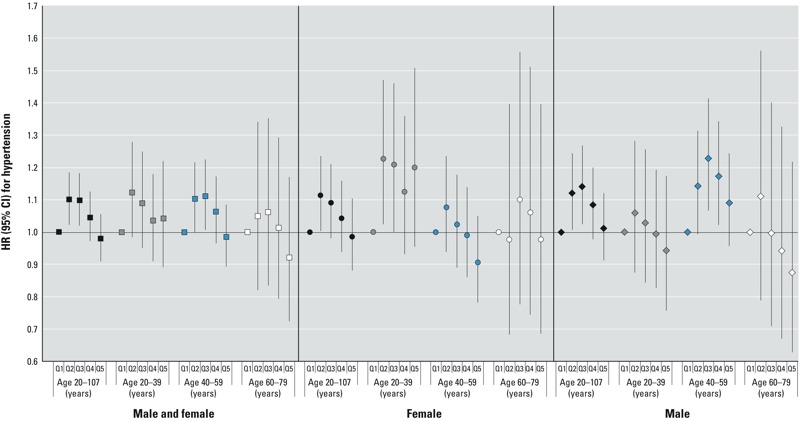
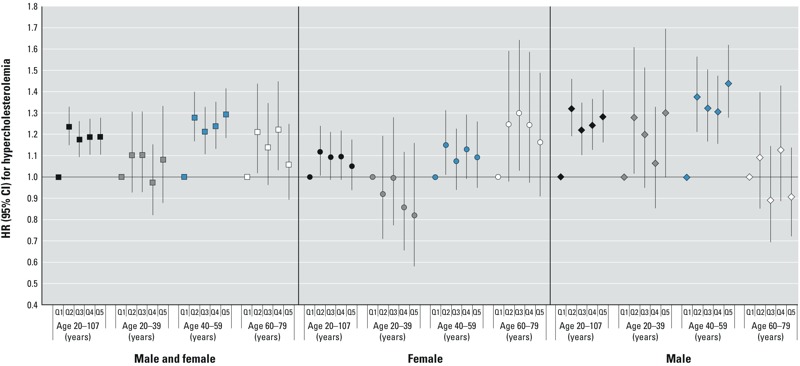
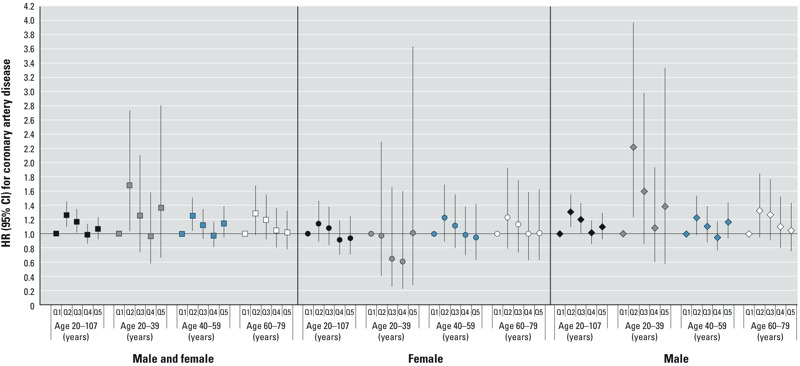
Results: Among 32,254 participants (28,541 community; 3,713 worker), 12,325 reported hypertension with medication, 9,909 reported hypercholesterolemia with medication, and 3,147 reported coronary artery disease (2,550 validated). Hypercholesterolemia incidence increased with increasing cumulative PFOA exposure (sum of yearly serum concentration estimates), most notably among males 40-60 years of age. Compared with the lowest exposure quintile (< 142 ng/mL-years), hazard ratios for subsequent quintiles (ng/mL-years: 142 to < 234; 234 to < 630; 630 to < 3,579; ≥ 3,579) were 1.24, 1.17, 1.19, and 1.19 overall and 1.38, 1.32, 1.31, and 1.44 among men 40-60 years of age. There was no apparent association between PFOA exposure and hypertension or coronary artery disease incidence.
Conclusions: Higher PFOA exposure was associated with incident hypercholesterolemia with medication, but not with hypertension or coronary artery disease.
Conflict of interest statement
The authors declare they have no actual or potential competing financial interests.
Figures
Comment in
-
PFOA and high cholesterol: basis for the finding of a probable link.Environ Health Perspect. 2014 Dec;122(12):A338. doi: 10.1289/ehp.122-A338. Environ Health Perspect. 2014. PMID: 25436834 Free PMC article. No abstract available.
References
-
- Costa G, Sartori S, Consonni D. Thirty years of medical surveillance in perfluooctanoic acid production workers. J Occup Environ Med. 2009;51:364–372. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
